Eating Disorder Awareness Week: Myth Busting
Eating disorder awareness week is very close to my heart. Having struggled with Anorexia Binge-Purge type in the past, I know how difficult life can be with an eating disorder. I’m also acutely aware of many myths and stereotypes about eating disorders, which can be hurtful to sufferers and can even put people off seeking treatment. So, in this article, I’ll talk about some common myths and stereotypes.
1. You have to be thin to have an eating disorder:
This is categorically not true. Many people with eating disorders are not underweight, as Anorexia represents only a minority of eating disorder cases, and is the only eating disorder clinically defined by being underweight. People with binge-eating disorder are often overweight/obese, and those with bulimia are often normal weight. Individuals who have an otherwise specified feeding or eating disorder (OSFED) or an eating disorder not otherwise specified (EDNOS), where symptoms don’t quite fall into either of the main eating disorder categories, can be any weight. Even people with anorexia don’t start off underweight; when I started losing weight I went from being at the high end of healthy weight to the low end, and was congratulated for losing ‘puppy fat’. I didn’t suddenly become sick when I went from a BMI of 18.5 to a BMI of 17; the behaviours I was using to lose weight were indicative of anorexia all along, even when I didn’t look sick.
2. Eating disorders only effect young girls:
While, statistically, anorexia is more common among women, anyone can be effected by an eating disorder. Rates of binge-eating disorder and bulimia are roughly equal between men and women, and typically start at an older age (20-25 for bulimia and 40+ for binge-eating disorder). Stereotypes about boys having less body image issues and being at less risk for an eating disorder can be very damaging, as they discourage boys (particularly teenage boys and young adults) from seeking help. Considering that people with anorexia have an 18x greater chance of committing suicide, and boys and young men are at increased risk of suicide relative to women and older men, a male with anorexia is very high risk and in need of help that they might be reluctant to seek.
Life stressors like pregnancy, divorce or the death of a loved one can also trigger a first episode or relapse of an eating disorder at any age. Older people can develop as severe an eating disorder as younger people, and their illness might not be recognised, putting them at a higher risk. Conversely, younger and younger children seem to be developing worrying signs of eating-disordered behaviours/thinking patterns, such as a focus on calories and not being ‘fat’.
3. People with eating disorders are attention seeking:
This is generally not true. Most people with eating disorders try very hard to hide their illness. In fact, people with bulimia and binge-eating disorder can go years without anyone knowing about their problems with food. People with anorexia generally cannot hide their illness as much as those with other eating disorders, because of the rapid weight loss often seen in anorexia. However, they will still use methods to try and hide their symptoms, such as wearing baggy tops and telling people that they have already eaten in order to avoid eating. Often individuals with eating disorders will become very angry and/or upset if they are ‘discovered’, and may vehemently deny that they have a problem. Many people with eating disorders actually do not feel that they have a problem, and this is especially true in anorexia, where individuals can have a distorted body image and be unable to see that they are ill.
On the other hand, there are some cases where eating disordered behaviours are used, consciously or unconsciously, to get attention. In these cases, individuals often display other attention seeking behaviour, such as ‘acting out’ by shouting/being aggressive or deliberately being caught doing self-destructive behaviours such as self-harm and purging. This is attention seeking. This does not make the person an ‘attention seeker’ in the derogative sense. Individuals who use attention seeking behaviour are often desperate, lonely and don’t know what to do. They might be crying out for help because they want to get better but don’t know how. They probably do need attention; if someone is engaging in very risky behaviours to get attention then they obviously aren’t getting enough/the right kind of attention. Sometimes an individual might have been emotionally neglected during childhood. In this case they may have used extreme behaviours as a child and learned that these get them attention, and so carried these types of behaviours into later life. It may be that the person hasn’t learned the skills to articulate their feelings, or deal with them appropriately, so they engage in risky behaviours and seek attention because they simply don’t know how else to cope. No one develops an eating disorder for the fun of it.
4. Anorexic individuals don’t ever eat:
Not true. There are two types of anorexia; restricting anorexia and binge-purge anorexia. The former type of anorexia does involve fasting and eating very little, but the second type of anorexia involves a pattern of overeating to excess (binging) and then compensating by throwing up/using laxatives/over-exercising/fasting. The latter type of anorexia is clinically very similar to bulimia, but individuals in this case are underweight, usually because they purge everything/almost everything that they eat. This form of anorexia, like all eating disorders, is very dangerous. People with anorexia binge-purge type have the health risks associated with being underweight/starved and with binging and purging, leading to electrolyte imbalances, possible long-term health effects like osteoporosis, and immediate risk to life. All of these risks can develop very quickly in someone who is starving and binging and purging.
5. People who aren’t underweight aren’t sick:
Nope. Individuals with bulimia are twice as likely to die as their ‘healthy’ counterparts. Bulimia can lead to electrolyte imbalances (caused by vomiting and laxative abuse), tooth decay, gastric problems and other health complications. An individual who is purging frequently is at a very high risk, no matter what their weight is.
People with binge-eating disorder can become obese, leading to the complications of obesity, such as heart disease and stroke.
Individuals who were obese and developed anorexia might remain at a high weight while starving themselves/engaging in dangerous behaviours to lose weight, and might become just as sick as someone who is severely underweight, due to rapid weight loss and malnutrition. Such a person might end up having a heart attack while being a perfectly healthy weight.
6. Eating disorders are all about weight and body image:
While many people with eating disorders (particularly anorexia and bulimia) do struggle with body image issues and weight obsession, there is a lot more to eating disorders than this. Many people with anorexia, for example, have traits of OCD and obsessive thinking, and have been ‘perfectionistic’ since childhood. This is known as a major risk factor for anorexia, and can remain part of a person’s personality after recovery. This perfectionism and obsessiveness can drive people to focus intensely on food and calories and reaching a ‘goal weight’.
Anxiety is another major risk factor for eating disorders. People might use food as a coping mechanism to calm their anxiety, whether that’s through binging, purging or restricting. I like to refer to this as ‘projecting anxiety onto food’. You might be worried about a relationship, or about work/school stress, and so start starving yourself because food provides a new focus for the anxiety which is more tangible and controllable. This links into another major factor in eating disorders; control. People who feel they have no control over their bodies/lives may use food as a way of regaining perceived control, as this might feel like the only thing they have control over.
There are also eating disorders which have nothing to do with body image and weight, such as avoidant restrictive feeding and eating disorder (ARFED), which is often triggered by a fear of choking/contamination. Unlike anorexia and bulimia, the diagnostic criteria for this disorder doesn’t involve body image issues or fear of weight gain, because some people with ARFED don’t have any body image issues, or the issues they do have are to do with being underweight and wanting to be able to put weight back on.
7. If someone is skinny they have anorexia:
While individuals who are underweight on purpose are likely to be diagnosed with anorexia, there are loads of reasons why someone might be skinny/underweight that have nothing to do with having an eating disorder. Some people are naturally skinny. Some people stop eating when they’re stressed, and their weight might actually be a sign of severe depression/anxiety rather than an eating disorder. Some people lose weight due to physical illness. It isn’t possible to look at someone and ‘know’ that they have an eating disorder. However, when it comes to long-term severe anorexia, it is almost always very obvious because the person will be very emaciated and skeletal.
8. When someone is weight restored they’re safe:
If someone is recovering from anorexia one of their main recovery goals will be to get back to a healthy weight. This will make them physically safer in terms of health risks, but it doesn’t necessarily mean they’re ‘all better’. In fact, from experience, I know that when someone first gets weight restored this can be a particularly risky time for a relapse, as well as other dangerous behaviours like self-harm and suicidal thoughts. When you’ve weight restored someone with anorexia you’ve basically taken away their coping mechanism, and made their eating disorder ‘voice’ very angry, and consequently, loud. Someone might reach a BMI of 19 and be physically a lot healthier than they were at an anorexic BMI, but their disordered thoughts might be the same, or even worse. They may still weigh their food, count calories, over-exercise and obsess over their weight, and so can be at a high risk of relapse. If a person with an eating disorder has not challenged their disordered thinking and been able to find alternative, healthy coping mechanisms, then it’s likely that they will fall back into old patterns of behaviour. In fact, many young people admitted into inpatient care with anorexia will put weight on while in hospital in order to be discharged, and will just lose it again after getting out. This is also true for bulimia, where people might stop their binging and purging behaviours while in inpatient care, but then continue these when they get out. This is because people might, frankly, ‘trick’ the system because they don’t want to be sectioned/kept in care. It could also be because an inpatient environment simply makes it easier to stop certain behaviours because you’re being watched all the time and pretty much forced to eat and not purge. When you get back into your old environment it’s very easy to fall back into eating disorder behaviours. This is especially true if there are stressors outside of inpatient care that can trigger the eating disorder.
Eating disorder awareness week is very close to my heart. Having struggled with Anorexia Binge-Purge type in the past, I know how difficult life can be with an eating disorder. I’m also acutely aware of many myths and stereotypes about eating disorders, which can be hurtful to sufferers and can even put people off seeking treatment. So, in this article, I’ll talk about some common myths and stereotypes.
1. You have to be thin to have an eating disorder:
This is categorically not true. Many people with eating disorders are not underweight, as Anorexia represents only a minority of eating disorder cases, and is the only eating disorder clinically defined by being underweight. People with binge-eating disorder are often overweight/obese, and those with bulimia are often normal weight. Individuals who have an otherwise specified feeding or eating disorder (OSFED) or an eating disorder not otherwise specified (EDNOS), where symptoms don’t quite fall into either of the main eating disorder categories, can be any weight. Even people with anorexia don’t start off underweight; when I started losing weight I went from being at the high end of healthy weight to the low end, and was congratulated for losing ‘puppy fat’. I didn’t suddenly become sick when I went from a BMI of 18.5 to a BMI of 17; the behaviours I was using to lose weight were indicative of anorexia all along, even when I didn’t look sick.
2. Eating disorders only effect young girls:
While, statistically, anorexia is more common among women, anyone can be effected by an eating disorder. Rates of binge-eating disorder and bulimia are roughly equal between men and women, and typically start at an older age (20-25 for bulimia and 40+ for binge-eating disorder). Stereotypes about boys having less body image issues and being at less risk for an eating disorder can be very damaging, as they discourage boys (particularly teenage boys and young adults) from seeking help. Considering that people with anorexia have an 18x greater chance of committing suicide, and boys and young men are at increased risk of suicide relative to women and older men, a male with anorexia is very high risk and in need of help that they might be reluctant to seek.
Life stressors like pregnancy, divorce or the death of a loved one can also trigger a first episode or relapse of an eating disorder at any age. Older people can develop as severe an eating disorder as younger people, and their illness might not be recognised, putting them at a higher risk. Conversely, younger and younger children seem to be developing worrying signs of eating-disordered behaviours/thinking patterns, such as a focus on calories and not being ‘fat’.
3. People with eating disorders are attention seeking:
This is generally not true. Most people with eating disorders try very hard to hide their illness. In fact, people with bulimia and binge-eating disorder can go years without anyone knowing about their problems with food. People with anorexia generally cannot hide their illness as much as those with other eating disorders, because of the rapid weight loss often seen in anorexia. However, they will still use methods to try and hide their symptoms, such as wearing baggy tops and telling people that they have already eaten in order to avoid eating. Often individuals with eating disorders will become very angry and/or upset if they are ‘discovered’, and may vehemently deny that they have a problem. Many people with eating disorders actually do not feel that they have a problem, and this is especially true in anorexia, where individuals can have a distorted body image and be unable to see that they are ill.
On the other hand, there are some cases where eating disordered behaviours are used, consciously or unconsciously, to get attention. In these cases, individuals often display other attention seeking behaviour, such as ‘acting out’ by shouting/being aggressive or deliberately being caught doing self-destructive behaviours such as self-harm and purging. This is attention seeking. This does not make the person an ‘attention seeker’ in the derogative sense. Individuals who use attention seeking behaviour are often desperate, lonely and don’t know what to do. They might be crying out for help because they want to get better but don’t know how. They probably do need attention; if someone is engaging in very risky behaviours to get attention then they obviously aren’t getting enough/the right kind of attention. Sometimes an individual might have been emotionally neglected during childhood. In this case they may have used extreme behaviours as a child and learned that these get them attention, and so carried these types of behaviours into later life. It may be that the person hasn’t learned the skills to articulate their feelings, or deal with them appropriately, so they engage in risky behaviours and seek attention because they simply don’t know how else to cope. No one develops an eating disorder for the fun of it.
4. Anorexic individuals don’t ever eat:
Not true. There are two types of anorexia; restricting anorexia and binge-purge anorexia. The former type of anorexia does involve fasting and eating very little, but the second type of anorexia involves a pattern of overeating to excess (binging) and then compensating by throwing up/using laxatives/over-exercising/fasting. The latter type of anorexia is clinically very similar to bulimia, but individuals in this case are underweight, usually because they purge everything/almost everything that they eat. This form of anorexia, like all eating disorders, is very dangerous. People with anorexia binge-purge type have the health risks associated with being underweight/starved and with binging and purging, leading to electrolyte imbalances, possible long-term health effects like osteoporosis, and immediate risk to life. All of these risks can develop very quickly in someone who is starving and binging and purging.
5. People who aren’t underweight aren’t sick:
Nope. Individuals with bulimia are twice as likely to die as their ‘healthy’ counterparts. Bulimia can lead to electrolyte imbalances (caused by vomiting and laxative abuse), tooth decay, gastric problems and other health complications. An individual who is purging frequently is at a very high risk, no matter what their weight is.
People with binge-eating disorder can become obese, leading to the complications of obesity, such as heart disease and stroke.
Individuals who were obese and developed anorexia might remain at a high weight while starving themselves/engaging in dangerous behaviours to lose weight, and might become just as sick as someone who is severely underweight, due to rapid weight loss and malnutrition. Such a person might end up having a heart attack while being a perfectly healthy weight.
6. Eating disorders are all about weight and body image:
While many people with eating disorders (particularly anorexia and bulimia) do struggle with body image issues and weight obsession, there is a lot more to eating disorders than this. Many people with anorexia, for example, have traits of OCD and obsessive thinking, and have been ‘perfectionistic’ since childhood. This is known as a major risk factor for anorexia, and can remain part of a person’s personality after recovery. This perfectionism and obsessiveness can drive people to focus intensely on food and calories and reaching a ‘goal weight’.
Anxiety is another major risk factor for eating disorders. People might use food as a coping mechanism to calm their anxiety, whether that’s through binging, purging or restricting. I like to refer to this as ‘projecting anxiety onto food’. You might be worried about a relationship, or about work/school stress, and so start starving yourself because food provides a new focus for the anxiety which is more tangible and controllable. This links into another major factor in eating disorders; control. People who feel they have no control over their bodies/lives may use food as a way of regaining perceived control, as this might feel like the only thing they have control over.
There are also eating disorders which have nothing to do with body image and weight, such as avoidant restrictive feeding and eating disorder (ARFED), which is often triggered by a fear of choking/contamination. Unlike anorexia and bulimia, the diagnostic criteria for this disorder doesn’t involve body image issues or fear of weight gain, because some people with ARFED don’t have any body image issues, or the issues they do have are to do with being underweight and wanting to be able to put weight back on.
7. If someone is skinny they have anorexia:
While individuals who are underweight on purpose are likely to be diagnosed with anorexia, there are loads of reasons why someone might be skinny/underweight that have nothing to do with having an eating disorder. Some people are naturally skinny. Some people stop eating when they’re stressed, and their weight might actually be a sign of severe depression/anxiety rather than an eating disorder. Some people lose weight due to physical illness. It isn’t possible to look at someone and ‘know’ that they have an eating disorder. However, when it comes to long-term severe anorexia, it is almost always very obvious because the person will be very emaciated and skeletal.
8. When someone is weight restored they’re safe:
If someone is recovering from anorexia one of their main recovery goals will be to get back to a healthy weight. This will make them physically safer in terms of health risks, but it doesn’t necessarily mean they’re ‘all better’. In fact, from experience, I know that when someone first gets weight restored this can be a particularly risky time for a relapse, as well as other dangerous behaviours like self-harm and suicidal thoughts. When you’ve weight restored someone with anorexia you’ve basically taken away their coping mechanism, and made their eating disorder ‘voice’ very angry, and consequently, loud. Someone might reach a BMI of 19 and be physically a lot healthier than they were at an anorexic BMI, but their disordered thoughts might be the same, or even worse. They may still weigh their food, count calories, over-exercise and obsess over their weight, and so can be at a high risk of relapse. If a person with an eating disorder has not challenged their disordered thinking and been able to find alternative, healthy coping mechanisms, then it’s likely that they will fall back into old patterns of behaviour. In fact, many young people admitted into inpatient care with anorexia will put weight on while in hospital in order to be discharged, and will just lose it again after getting out. This is also true for bulimia, where people might stop their binging and purging behaviours while in inpatient care, but then continue these when they get out. This is because people might, frankly, ‘trick’ the system because they don’t want to be sectioned/kept in care. It could also be because an inpatient environment simply makes it easier to stop certain behaviours because you’re being watched all the time and pretty much forced to eat and not purge. When you get back into your old environment it’s very easy to fall back into eating disorder behaviours. This is especially true if there are stressors outside of inpatient care that can trigger the eating disorder.
So What about Depression?
Depression is a mood disorder characterised by emotional, psychological and physical symptoms, including:
Depression is much more than feeling sad. Here’s a little story to help clarify the difference:
Jo is feeling unhappy because she got a bad grade on a test. She’s a little tearful and thinks it’s her fault. She is upset for a few hours and talks to her mum. After a while her mum is able to reassure her and make her feel better. She decides to try harder on her next test.
Ashley is feeling very guilty. She got a bad grade on a test. She cries and stays by herself. When her mum tries to talk to her she shouts at her to go away because she doesn’t want to see anyone. She feels physically sick and is unable to stop crying for a long time. She has thoughts like “I’m such an idiot”, “I always fail”, “I’m worthless”, which make her feel helpless and alone. She has the urge to harm herself. After weeks Ashley is still struggling, and sometimes feels very numb and ‘strange’, like she isn’t real. Other times she feels very, very sad, like there’s a black hole about to swallow her up. She doesn’t sleep very well and doesn’t enjoy food or spending time with her friends, even though she used to be really sociable. Other people notice that she’s not herself and are worried about her.
So, in depression, people’s reactions to negative events can be very extreme. Although everyone gets sad sometimes, people with depression experience such an intense sadness that they often feel they can’t go on with their life. For some people it can feel like a physical pain in their chest/stomach that just won’t go away, like the sinking feeling you might get if you saw your crush kiss someone else, but all the time. It might help to think about how a depression in a mountainside looks like a piece of the mountain has sunk into itself. People with depression have sunk, physically, mentally and emotionally.
Everyone experiences depression differently; some people get extremely irritable, while others become very sad. Some people become socially withdrawn, while others remain social, going through the motions at work and with friends, trying to remain ‘normal’. Some people experience depression triggered by an event, like a divorce or death of a loved one, while other people cannot pinpoint an event that triggered their depression.
Something all people with depression have in common is a set of debilitating symptoms that often interfere with their ability to function in everyday life, and can even put their life at risk (e.g. suicidal ideations). People with ‘high functioning depression’, who are able to maintain work and a social life, often feel that they aren’t ‘properly depressed’. This is a dangerous misconception; people who put the pressure on themselves to put a brave face on, despite feeling depressed, often end up breaking down when they are no longer able to hide their symptoms.
Women are statistically more likely than men to experience depression. This might be due to estrogen, especially since men in their 50’s are at a higher risk of depression at the same time testosterone levels drop. It is also possible that men are less likely to report and seek help for depression, due to stereotypes about masculinity, such as ‘a real man doesn’t cry’ and statements like ‘man up’. This is a scary possibility given that suicide rates in 2015 were 75% male (https://www.thecalmzone.net/help/get-help/suicide/). This might be due to the fact that, even though women attempt suicide more, men use more violent means and are less likely to be stopped. Additionally, men might feel less able to speak openly about suicidal thoughts and depression than women, since women are stereo-typically more emotional and depression is often seen as a ‘woman’s’ illness. On the other hand, it is also possible that women do experience depression more often, potentially due to higher rates of sexual and physical abuse (risk factors for depression) in girls, and higher rates of Anorexia, a severe eating disorder which can lead to depressive symptoms due to malnutrition, in girls.
Whatever the reason for the statistics, it’s clear that both men and women can suffer greatly due to depression, and that both need help to speak up and get help. Tackling stigma, as well as stereotypes about what a ‘real man’ should be like, could encourage men with depression to speak out. Equally, early interventions for both male and female victims of sexual and physical abuse might help prevent some depressive disorders.
While it is often believed that depression mostly affects teenagers, it can influence anyone at any stage in their life. It can even influence foetal development; depressed women are more likely to give birth early, increasing health risks for both the mother and the baby. Furthermore, between 14 and 23% of pregnant women experience some sort of depressive disorder. Having a depressed mother also increases your chances of developing depression yourself. Most people who get depression develop it in their twenties, but even children can be clinically depressed.
One of the scariest statistics to do with depression is that, In 2014, 19.7% of people in the UK aged 16 and over showed symptoms of anxiety or depression (https://www.mentalhealth.org.uk/). That's a lot of people. Given that suicide is a high risk in many depressive disorders, it is concerning that the prevalence of depression is so high. It's also worrying to know that 1 in 15 people have made an attempt on their life, and suicide is the most common cause of death for men aged 20-49 years in England and Wales (https://www.mentalhealth.org.uk/).
It can be very hard to ever understand why someone would want to take their own life. If you've never been suicidal then it's likely death seems like such a terrifying thing to you that you cannot imagine ever wanting it. Something to remember is that many people who feel suicidal don't necessarily want death, it just feels like their only option because of how painful life feels to them. Excuse the metaphors, but I think they’re useful, so here’s another one from J.K. Rowling that you’re probably familiar with; the Dementors. J.K states she based these creatures on her experience of depression. They feel on painful memories and suck the happiness and life right out of a person. Being attacked by a Dementor can make you feel like you don't even want to live anymore. This is what depression can do to a person; cause them so much pain that they become suicidal. The more painful memories you have, the more Dementors can hurt you, but focusing on happy memories can help you fight them. I think this is a helpful way of thinking about depression; painful memories can leave you feeling lifeless and without hope or happiness, but focusing on happy memories can help you to recover.
If you’re as yet unconvinced that depression is a ‘real’ illness, take a moment to consider this: people with depression are more likely to have chronic illnesses, chronic pain (especially back and neck pain), and often have predictable patterns of difficulty sleeping and early waking. Importantly, a depressed brain looks different than a non-depressed brain; MRI scans and other brain imaging techniques suggest the structure and brain circuits of depressed brains are different than those of non-depressed brains. Effected areas include the frontal lobe and the amygdala, areas of the brain linked to cognitive ability/reasoning and emotion regulation, respectively. This makes sense when we look at symptoms like difficulty concentrating and chronic sadness.
If you are feeling suicidal or like you don't know where to turn, please call one of these helplines/talk to someone you trust:
The Samaritons: 116 123
CALM: 0800 58 58 58
Childline: 0800 1111
Useful links:
https://www.psychologytoday.com/gb/blog/emotional-fitness/200907/10-little-known-facts-about-depression
https://www.everydayhealth.com/hs/major-depression-health-well-being/surprising-depression-facts/
https://www.hopefordepression.org/depression-facts/
https://www.factinate.com/things/40-facts-depression/
Depression is a mood disorder characterised by emotional, psychological and physical symptoms, including:
- Chronic feelings of sadness.
- Feelings of worthlessness and helplessness.
- Feelings of guilt.
- Irritability.
- Chronic pain/illness.
- Difficulty sleeping (hypo/hypersomnia; sleeping too much or not enough).
- Early waking.
- Low self-esteem.
- Social withdrawal.
- Fatigue and chronic tiredness.
- Thoughts of harming oneself/suicide.
- Self-harm.
- Plans of suicide/attempted suicide.
- Changes in appetite (loss of appetite is most common).
- Unexpected weight changes (e.g. losing a lot of weight without trying).
- Feeling numb (emotionless and detached from the world).
- Loss of enjoyment in activities one used to like.
- Difficulty concentrating.
Depression is much more than feeling sad. Here’s a little story to help clarify the difference:
Jo is feeling unhappy because she got a bad grade on a test. She’s a little tearful and thinks it’s her fault. She is upset for a few hours and talks to her mum. After a while her mum is able to reassure her and make her feel better. She decides to try harder on her next test.
Ashley is feeling very guilty. She got a bad grade on a test. She cries and stays by herself. When her mum tries to talk to her she shouts at her to go away because she doesn’t want to see anyone. She feels physically sick and is unable to stop crying for a long time. She has thoughts like “I’m such an idiot”, “I always fail”, “I’m worthless”, which make her feel helpless and alone. She has the urge to harm herself. After weeks Ashley is still struggling, and sometimes feels very numb and ‘strange’, like she isn’t real. Other times she feels very, very sad, like there’s a black hole about to swallow her up. She doesn’t sleep very well and doesn’t enjoy food or spending time with her friends, even though she used to be really sociable. Other people notice that she’s not herself and are worried about her.
So, in depression, people’s reactions to negative events can be very extreme. Although everyone gets sad sometimes, people with depression experience such an intense sadness that they often feel they can’t go on with their life. For some people it can feel like a physical pain in their chest/stomach that just won’t go away, like the sinking feeling you might get if you saw your crush kiss someone else, but all the time. It might help to think about how a depression in a mountainside looks like a piece of the mountain has sunk into itself. People with depression have sunk, physically, mentally and emotionally.
Everyone experiences depression differently; some people get extremely irritable, while others become very sad. Some people become socially withdrawn, while others remain social, going through the motions at work and with friends, trying to remain ‘normal’. Some people experience depression triggered by an event, like a divorce or death of a loved one, while other people cannot pinpoint an event that triggered their depression.
Something all people with depression have in common is a set of debilitating symptoms that often interfere with their ability to function in everyday life, and can even put their life at risk (e.g. suicidal ideations). People with ‘high functioning depression’, who are able to maintain work and a social life, often feel that they aren’t ‘properly depressed’. This is a dangerous misconception; people who put the pressure on themselves to put a brave face on, despite feeling depressed, often end up breaking down when they are no longer able to hide their symptoms.
Women are statistically more likely than men to experience depression. This might be due to estrogen, especially since men in their 50’s are at a higher risk of depression at the same time testosterone levels drop. It is also possible that men are less likely to report and seek help for depression, due to stereotypes about masculinity, such as ‘a real man doesn’t cry’ and statements like ‘man up’. This is a scary possibility given that suicide rates in 2015 were 75% male (https://www.thecalmzone.net/help/get-help/suicide/). This might be due to the fact that, even though women attempt suicide more, men use more violent means and are less likely to be stopped. Additionally, men might feel less able to speak openly about suicidal thoughts and depression than women, since women are stereo-typically more emotional and depression is often seen as a ‘woman’s’ illness. On the other hand, it is also possible that women do experience depression more often, potentially due to higher rates of sexual and physical abuse (risk factors for depression) in girls, and higher rates of Anorexia, a severe eating disorder which can lead to depressive symptoms due to malnutrition, in girls.
Whatever the reason for the statistics, it’s clear that both men and women can suffer greatly due to depression, and that both need help to speak up and get help. Tackling stigma, as well as stereotypes about what a ‘real man’ should be like, could encourage men with depression to speak out. Equally, early interventions for both male and female victims of sexual and physical abuse might help prevent some depressive disorders.
While it is often believed that depression mostly affects teenagers, it can influence anyone at any stage in their life. It can even influence foetal development; depressed women are more likely to give birth early, increasing health risks for both the mother and the baby. Furthermore, between 14 and 23% of pregnant women experience some sort of depressive disorder. Having a depressed mother also increases your chances of developing depression yourself. Most people who get depression develop it in their twenties, but even children can be clinically depressed.
One of the scariest statistics to do with depression is that, In 2014, 19.7% of people in the UK aged 16 and over showed symptoms of anxiety or depression (https://www.mentalhealth.org.uk/). That's a lot of people. Given that suicide is a high risk in many depressive disorders, it is concerning that the prevalence of depression is so high. It's also worrying to know that 1 in 15 people have made an attempt on their life, and suicide is the most common cause of death for men aged 20-49 years in England and Wales (https://www.mentalhealth.org.uk/).
It can be very hard to ever understand why someone would want to take their own life. If you've never been suicidal then it's likely death seems like such a terrifying thing to you that you cannot imagine ever wanting it. Something to remember is that many people who feel suicidal don't necessarily want death, it just feels like their only option because of how painful life feels to them. Excuse the metaphors, but I think they’re useful, so here’s another one from J.K. Rowling that you’re probably familiar with; the Dementors. J.K states she based these creatures on her experience of depression. They feel on painful memories and suck the happiness and life right out of a person. Being attacked by a Dementor can make you feel like you don't even want to live anymore. This is what depression can do to a person; cause them so much pain that they become suicidal. The more painful memories you have, the more Dementors can hurt you, but focusing on happy memories can help you fight them. I think this is a helpful way of thinking about depression; painful memories can leave you feeling lifeless and without hope or happiness, but focusing on happy memories can help you to recover.
If you’re as yet unconvinced that depression is a ‘real’ illness, take a moment to consider this: people with depression are more likely to have chronic illnesses, chronic pain (especially back and neck pain), and often have predictable patterns of difficulty sleeping and early waking. Importantly, a depressed brain looks different than a non-depressed brain; MRI scans and other brain imaging techniques suggest the structure and brain circuits of depressed brains are different than those of non-depressed brains. Effected areas include the frontal lobe and the amygdala, areas of the brain linked to cognitive ability/reasoning and emotion regulation, respectively. This makes sense when we look at symptoms like difficulty concentrating and chronic sadness.
If you are feeling suicidal or like you don't know where to turn, please call one of these helplines/talk to someone you trust:
The Samaritons: 116 123
CALM: 0800 58 58 58
Childline: 0800 1111
Useful links:
https://www.psychologytoday.com/gb/blog/emotional-fitness/200907/10-little-known-facts-about-depression
https://www.everydayhealth.com/hs/major-depression-health-well-being/surprising-depression-facts/
https://www.hopefordepression.org/depression-facts/
https://www.factinate.com/things/40-facts-depression/

Helping someone with an eating disorder over Christmas
Christmas can be a really difficult time for anyone suffering from, or recovering from, an eating disorder. There’s so much food, routines are disrupted, and portions are big. It can be analogous to throwing someone with arachnophobia into a pit of spiders, and then expecting them to be jolly. For families and loved ones, too, it can be stressful. Not knowing how to react, or to help, a loved one with an eating disorder over Christmas, can feel like an extra pressure. This article will outline just why Christmas can be so tricky for someone with an eating disorder, and how you can help.
Difficulty One: Portion sizes- portion sizes over Christmas are often, let’s say, generous. This can be very stressful for someone with eating difficulties. Being surrounded by a large amount of food can trigger urges to binge, purge and starve oneself. For people with a history of binging and purging behaviours this can be particularly poignant; the sheer amount of food a person is expected to eat over Christmas can make a person feel like their binging. For people who count calories and/or restrict their food intake, the amount of food can be extremely anxiety provoking, because it triggers a deep-routed fear of food and weight gain. If an individual is unable to control how much food they will be given, or expected to have, this can be even harder. This is because many people with eating disorders (especially anorexia) use their eating behaviours to gain a sense of control, and are very uncomfortable if they cannot do this.
How to help: you can help someone with an eating disorder with portion sizes by letting them choose what, and how much, they have. If the Christmas dinner is being self-served then consider having the food separate from where you’re eating, so that your loved one doesn’t have to be surrounded by food while they’re eating, and so they won’t feel quite as ‘watched’ while they’re getting their food. Letting the person help with the cooking can be helpful as well; they can feel a greater sense of control over their food as they’ll know what’s in it. On the other hand, watching food being prepared can also be stressful for some individuals with eating disorders, particularly if they’re watching someone put oil and the like on their food. Discuss with the person what they feel will make them most comfortable.
Difficulty Two: diet/calorie talk- over Christmas diet talk, and focus on calories, can increase. Many people talk about how they’re ‘going to have to work off their dinner’, or how they’re not having as much because they don’t want to gain weight. A lot of people might also say things like ‘this has a lot of calories’ or ‘there’s so much food’. While these comments won’t be intended badly, talk about calories and food can make people very uncomfortable and can be triggering. This is because many individuals with eating disorders think a lot about calories and have to work hard to loosen up with regards to rigid dietary rules. Diet and calorie talk can make people feel guilty about eating, and can trigger urges to purge/starve. Try to remember that, for a lot of people with eating disorders, their eating disorder ‘voice’ can be like an extreme dieter; constantly urging the person not to eat/to engage in extreme methods to lose weight. It is also a harsh critic, which will take any excuse to tell the person what an awful human being they are. Any focus on what the person is eating/how much they’re eating, can be fuel for their inner critic.
How to help: try to limit any talk about weight/food/calories. It’s a holiday, not backstage a catwalk. It can be helpful to encourage discussion about things that will distract your loved one from thinking about what they’re eating. You could talk about presents, party games, music. Basically anything but food/body image. If someone brings up the topic of dieting/calories, it can be helpful to counteract it with statements like “personally I don’t worry about that because I know it doesn’t really matter”, and swiftly move the conversation on.
Difficulty Three: disrupted routines- often when people are recovering from an eating disorder routines around food are very important. When routines are disrupted it can be very distressing and can cause people to want to stray from their meal plan, which can encourage lapses. During Christmas eating routines are, frankly, completely messed up. People eat turkey sandwiches at nine in the morning, and have dinner at lunchtime. It’s like the world gets turned upside down, which is not easy for someone with an eating disorder.
How to help: try talking to your loved one before Christmas about when they want to have Christmas dinner and consider helping them with a Christmas meal plan so that they can prepare themselves before. Simply letting a person know when the Christmas meal will be happening can ease their anxiety. Give the person a choice about when they want to eat; if they want to eat separately to other people try to understand and let them do what’s best for them. Encouraging the person, gently, to eat enough, and to eat with the family, is good. However, pressuring your loved one may make them more likely to withdraw back into their eating disorder mind-set.
Difficulty Four: if a person is still ill/relapses- this is basically worse-case scenario. If your loved one is still in the midst of their eating disorder it is likely that Christmas may feel nightmarish, for them and you. If this is your situation then I would suggest that you signpost your loved one to online support and take them to their GP as soon as possible. In this case, it is likely to be best for the individual to not eat the same as everyone else on Christmas, as this could cause an increase in eating disordered thoughts and behaviours. You may find that, if your loved one has a problem with binging, this gets worse over the holidays. This is the same if they have a problem with purging. Don’t despair, it is unfortunate, but to be expected.
How to help: if your loved one relapses during Christmas try to remind them of strategies they used before to get better. Be as supportive as possible and let them know you’re there for them. It’s horrible if someone close to you becomes ill in this way, but try to remember that you can only support them, you cannot fix them. Try to enjoy the holidays as much as possible, and don’t put pressure on yourself to make everything right. If your loved one has never had treatment before, and is ill during the holidays, it might be helpful to get informed by going online to sites like BEAT and YoungMinds. Try to get your loved one help as soon as possible. It can be difficult to get into services during the Christmas period, so during this time it might be helpful to find any online support to get your loved one through until the New Year. If you’re worried about their immediate health/safety then take the individual to hospital. Warning signs include; a weak pulse, fainting and sharp abdominal pain.
Remember to take care of yourself as well. Christmas can be a stressful time for everyone, whether you’ve got an eating disorder or not. Trying to support someone who is struggling is noble, and also tricky at times. Cut yourself some slack and remember that, if you’re being as supportive and understanding as you can, you’re doing brilliantly.
Christmas can be a really difficult time for anyone suffering from, or recovering from, an eating disorder. There’s so much food, routines are disrupted, and portions are big. It can be analogous to throwing someone with arachnophobia into a pit of spiders, and then expecting them to be jolly. For families and loved ones, too, it can be stressful. Not knowing how to react, or to help, a loved one with an eating disorder over Christmas, can feel like an extra pressure. This article will outline just why Christmas can be so tricky for someone with an eating disorder, and how you can help.
Difficulty One: Portion sizes- portion sizes over Christmas are often, let’s say, generous. This can be very stressful for someone with eating difficulties. Being surrounded by a large amount of food can trigger urges to binge, purge and starve oneself. For people with a history of binging and purging behaviours this can be particularly poignant; the sheer amount of food a person is expected to eat over Christmas can make a person feel like their binging. For people who count calories and/or restrict their food intake, the amount of food can be extremely anxiety provoking, because it triggers a deep-routed fear of food and weight gain. If an individual is unable to control how much food they will be given, or expected to have, this can be even harder. This is because many people with eating disorders (especially anorexia) use their eating behaviours to gain a sense of control, and are very uncomfortable if they cannot do this.
How to help: you can help someone with an eating disorder with portion sizes by letting them choose what, and how much, they have. If the Christmas dinner is being self-served then consider having the food separate from where you’re eating, so that your loved one doesn’t have to be surrounded by food while they’re eating, and so they won’t feel quite as ‘watched’ while they’re getting their food. Letting the person help with the cooking can be helpful as well; they can feel a greater sense of control over their food as they’ll know what’s in it. On the other hand, watching food being prepared can also be stressful for some individuals with eating disorders, particularly if they’re watching someone put oil and the like on their food. Discuss with the person what they feel will make them most comfortable.
Difficulty Two: diet/calorie talk- over Christmas diet talk, and focus on calories, can increase. Many people talk about how they’re ‘going to have to work off their dinner’, or how they’re not having as much because they don’t want to gain weight. A lot of people might also say things like ‘this has a lot of calories’ or ‘there’s so much food’. While these comments won’t be intended badly, talk about calories and food can make people very uncomfortable and can be triggering. This is because many individuals with eating disorders think a lot about calories and have to work hard to loosen up with regards to rigid dietary rules. Diet and calorie talk can make people feel guilty about eating, and can trigger urges to purge/starve. Try to remember that, for a lot of people with eating disorders, their eating disorder ‘voice’ can be like an extreme dieter; constantly urging the person not to eat/to engage in extreme methods to lose weight. It is also a harsh critic, which will take any excuse to tell the person what an awful human being they are. Any focus on what the person is eating/how much they’re eating, can be fuel for their inner critic.
How to help: try to limit any talk about weight/food/calories. It’s a holiday, not backstage a catwalk. It can be helpful to encourage discussion about things that will distract your loved one from thinking about what they’re eating. You could talk about presents, party games, music. Basically anything but food/body image. If someone brings up the topic of dieting/calories, it can be helpful to counteract it with statements like “personally I don’t worry about that because I know it doesn’t really matter”, and swiftly move the conversation on.
Difficulty Three: disrupted routines- often when people are recovering from an eating disorder routines around food are very important. When routines are disrupted it can be very distressing and can cause people to want to stray from their meal plan, which can encourage lapses. During Christmas eating routines are, frankly, completely messed up. People eat turkey sandwiches at nine in the morning, and have dinner at lunchtime. It’s like the world gets turned upside down, which is not easy for someone with an eating disorder.
How to help: try talking to your loved one before Christmas about when they want to have Christmas dinner and consider helping them with a Christmas meal plan so that they can prepare themselves before. Simply letting a person know when the Christmas meal will be happening can ease their anxiety. Give the person a choice about when they want to eat; if they want to eat separately to other people try to understand and let them do what’s best for them. Encouraging the person, gently, to eat enough, and to eat with the family, is good. However, pressuring your loved one may make them more likely to withdraw back into their eating disorder mind-set.
Difficulty Four: if a person is still ill/relapses- this is basically worse-case scenario. If your loved one is still in the midst of their eating disorder it is likely that Christmas may feel nightmarish, for them and you. If this is your situation then I would suggest that you signpost your loved one to online support and take them to their GP as soon as possible. In this case, it is likely to be best for the individual to not eat the same as everyone else on Christmas, as this could cause an increase in eating disordered thoughts and behaviours. You may find that, if your loved one has a problem with binging, this gets worse over the holidays. This is the same if they have a problem with purging. Don’t despair, it is unfortunate, but to be expected.
How to help: if your loved one relapses during Christmas try to remind them of strategies they used before to get better. Be as supportive as possible and let them know you’re there for them. It’s horrible if someone close to you becomes ill in this way, but try to remember that you can only support them, you cannot fix them. Try to enjoy the holidays as much as possible, and don’t put pressure on yourself to make everything right. If your loved one has never had treatment before, and is ill during the holidays, it might be helpful to get informed by going online to sites like BEAT and YoungMinds. Try to get your loved one help as soon as possible. It can be difficult to get into services during the Christmas period, so during this time it might be helpful to find any online support to get your loved one through until the New Year. If you’re worried about their immediate health/safety then take the individual to hospital. Warning signs include; a weak pulse, fainting and sharp abdominal pain.
Remember to take care of yourself as well. Christmas can be a stressful time for everyone, whether you’ve got an eating disorder or not. Trying to support someone who is struggling is noble, and also tricky at times. Cut yourself some slack and remember that, if you’re being as supportive and understanding as you can, you’re doing brilliantly.
Glamorizing Mental Illness
Glamorizing mental illness is a difficult and frustrating topic. On the one hand, I want to say that anything which raises awareness for mental health issues is doing a good thing; people often find it difficult to talk about these things, so having TV shows/movies/books which talk about mental health can be helpful. On the other hand, certain portrayals of mental illness can trivialize it, and even make it seem attractive. For example, in 13 Reasons Why, there are quite a few problematic scenes. The fact that after her suicide Hannah is given attention, and the people she sends tapes to show their regret for what they did to her, could make it seem like suicide is a way to get people to care. This plus the graphic scene depicting Hannah’s actual suicide can be both triggering and glamorizing. There are good points to this show; it deals with sexual assault/rape, bullying and mental health problems. It also shows how things that seem ‘small’ can all pile up and make life unbearable for some people. However, the triggering nature of some of its contents, and the fact that Hannah ‘lives on’ through her tapes, may be problematic, so I would warn people in a bad place to avoid the show until they feel that they won’t be too affected by it.
A film/book that deals with suicide in, what I feel, is a less triggering and glamorizing way, is It’s Kind of a Funny Story. This is about a young man, Craig, who goes to the emergency department after feeling depressed and suicidal. He’s admitted to a mental health ward, where he meets other people going through mental illness, and is able to talk to a therapist, and his new friends, about why he’s struggling. He uses his art and the wisdom of the people in the ward to form a new perspective on life and gain hope. At the end, although he obviously still has problems, he’s hopeful and feels able to move on in life. This is based on a true story and is both funny and heart-warming. Although there is discussion of suicide (one of the characters has attempted suicide many times), and one of the characters has self-harm scars, there is no graphic depiction of suicide or self-harm, making this less triggering than some other shows/movies.
One depiction of mental illness I was conflicted about was To The Bone. This Netflix film was written by, and had input from, people who’ve suffered with eating disorders. The main character, Ellen/Eli, is a 20-year-old woman who suffers from Anorexia Nervosa. I was scared to watch this honestly, because I’d heard about it before and knew that the actress had previously suffered from an eating disorder. The fact that she had to lose weight for the role, considering what she’s been through, is scary, even though she did have doctors around her. I know how triggering weight loss can be for an eating disorder even when it’s not expected, let alone when it is. Aside from that, I actually thought the film was a really accurate and heart wrenching depiction of Anorexia. I liked that there was never a reason given for why Eli had an eating disorder; there were lots of things that might have contributed, but none that were overly focused on. She says she doesn’t really know why she keeps doing it, and I think that sometimes anyone suffering from an eating disorder can feel that way; ending up in a cycle and getting so used to the behavior that doing anything else feels alien.
One of the staff at the group home where Eli ends up points out that what the people there are doing is trying to numb themselves from things they don’t want to feel, and this I think is really true for a lot of people with eating disorders. So when, after having an argument with her new friend, Eli starts doing vigorous sit-ups, it’s fairly clear this is one of her ways of coping. Another good thing about this show was the depiction of a boy recovering from Anorexia, who seems to act as a source of hope and says things like “feel the fear and do it anyway” when encouraging Eli to eat. Although he does pressure her to eat, saying things like “coward”, which, obviously enough, doesn’t make her suddenly able to eat.
Different ways that families might deal with their daughter/son, sister/brother, etc., having an eating disorder are depicted. For example, Eli’s step-mum takes a picture of Eli’s emancipated body to show her, saying “do you think that’s beautiful?”, and also bakes her a cake with “eat up Ellen” written on it, showing how sometimes people don’t always approach eating disorders in the most tactful way. It’s also clear that she cares a lot for Ellen, organizing for her to see doctors and get inpatient treatment, trying to encourage her to eat. I think this shows how, even when parents/friends/siblings aren’t so helpful, they can still be trying really hard in their own way. So, while this movie is massively triggering for anyone who’s dealt with/is dealing with an eating disorder, it’s also really informative and heartfelt, and real too. That’s why I would recommend, with caution, that people watch this movie and take in what Eli’s going through, but please don’t watch it if you think it will make eating disordered thoughts/behaviors worse.
Mental illness is often glamorized on social media sites like Tumblr. While the site has gotten a lot better for this since I was a teenager, with loads of wonderful blogs encouraging recovery and giving tips for improving self-esteem, there are still some things that worry me. Some content, while not necessarily intending to glamorize mental illness, does perpetuate eating disordered ideas. I’m talking about ‘thinspiration’. This includes images and quotes designed to encourage people to lose weight/not eat, such as “skip dinner, wake up thinner”, as well as pictures of very thin girls/people with severe anorexia, with comments from individuals saying things like “I wish I looked like that”, “so beautiful”,
Tumblr’s tried hard to deal with ‘thinspiration’, for example, a message comes up referring you to helplines if you type in anything to do with thinspiration. Unfortunately, there’s always ways around these things, and thinspiration is still rife under different names (plus you can still continue to content after a warning).
Much of the online ana/mia (anorexia/bulimia) community perpetuates the idea of eating disorders being a ‘lifestyle choice’ and a sign of strength, which is, needless to say, very dangerous. Now, I don’t want to demonize the online eating disorder community; these people are suffering enough. I do want to warn against entering it though. The people who post thinspiration content and ‘eating disorder tips’ are usually very ill and looking for people who understand them, or even just a justification for their behaviors and feelings. The content posted under the veil of mental illness can be damaging to young minds. Some people aren’t able to see that thinspiration is often produced by people feeling intense sadness and fear. This isn’t helped by the fact that non-anorexic ‘thinspiration’ is pretty much everywhere. If you look up healthy lifestyle on Pinterest, you’ll get pictures of skinny women with unrealistically flat stomachs and abs (these woman are probably personal trainers/go to the gym every day), as well as weight loss tips and exercises for a ‘better body’. Obviously, there’s a lot of great body positive stuff out there, but when there’s such an emphasis on being skinny/ ‘ripped’, it shouldn’t be surprising that a lot of young people end up feeling bad about their bodies and can become at risk of getting an eating disorder. So, when there’s also content that explicitly encourages and even gives ‘tips’ for eating disorders it can be really damaging.
It can be difficult for institutions and individuals trying to create content about mental illness without glamorizing it, especially when it comes to movies/TV shows; they need to be entertaining. Not being an expert, I can’t say how to make good content about mental illness, but I think a lot of content makers know that they need to do their research to make a realistic depiction. I also think humor is so, so important; if you’re going to break our hearts at least throw in a joke. It can’t be easy to make media about mental health, so I applaud anyone who does. However, if it becomes glamorizing/triggering, then it might not serve the purpose for which it was intended.
Sometimes mental illness is glamorized as ‘tragically beautiful’, or ‘special’, and I don’t want to disrespect other people’s creativity and/or ways of coping, but I just think it’s untrue to depict mental illness as anything but painful and sucky. So, let’s glamorize health and happiness. Let’s glamorize being able to just eat a chocolate bar without feeling like the world’s ending. Let’s glamorize being able to go out and have a good time with friends, instead of sitting alone in pain. Let’s glamorize strength and resilience. Let’s glamorize recovery.
Glamorizing mental illness is a difficult and frustrating topic. On the one hand, I want to say that anything which raises awareness for mental health issues is doing a good thing; people often find it difficult to talk about these things, so having TV shows/movies/books which talk about mental health can be helpful. On the other hand, certain portrayals of mental illness can trivialize it, and even make it seem attractive. For example, in 13 Reasons Why, there are quite a few problematic scenes. The fact that after her suicide Hannah is given attention, and the people she sends tapes to show their regret for what they did to her, could make it seem like suicide is a way to get people to care. This plus the graphic scene depicting Hannah’s actual suicide can be both triggering and glamorizing. There are good points to this show; it deals with sexual assault/rape, bullying and mental health problems. It also shows how things that seem ‘small’ can all pile up and make life unbearable for some people. However, the triggering nature of some of its contents, and the fact that Hannah ‘lives on’ through her tapes, may be problematic, so I would warn people in a bad place to avoid the show until they feel that they won’t be too affected by it.
A film/book that deals with suicide in, what I feel, is a less triggering and glamorizing way, is It’s Kind of a Funny Story. This is about a young man, Craig, who goes to the emergency department after feeling depressed and suicidal. He’s admitted to a mental health ward, where he meets other people going through mental illness, and is able to talk to a therapist, and his new friends, about why he’s struggling. He uses his art and the wisdom of the people in the ward to form a new perspective on life and gain hope. At the end, although he obviously still has problems, he’s hopeful and feels able to move on in life. This is based on a true story and is both funny and heart-warming. Although there is discussion of suicide (one of the characters has attempted suicide many times), and one of the characters has self-harm scars, there is no graphic depiction of suicide or self-harm, making this less triggering than some other shows/movies.
One depiction of mental illness I was conflicted about was To The Bone. This Netflix film was written by, and had input from, people who’ve suffered with eating disorders. The main character, Ellen/Eli, is a 20-year-old woman who suffers from Anorexia Nervosa. I was scared to watch this honestly, because I’d heard about it before and knew that the actress had previously suffered from an eating disorder. The fact that she had to lose weight for the role, considering what she’s been through, is scary, even though she did have doctors around her. I know how triggering weight loss can be for an eating disorder even when it’s not expected, let alone when it is. Aside from that, I actually thought the film was a really accurate and heart wrenching depiction of Anorexia. I liked that there was never a reason given for why Eli had an eating disorder; there were lots of things that might have contributed, but none that were overly focused on. She says she doesn’t really know why she keeps doing it, and I think that sometimes anyone suffering from an eating disorder can feel that way; ending up in a cycle and getting so used to the behavior that doing anything else feels alien.
One of the staff at the group home where Eli ends up points out that what the people there are doing is trying to numb themselves from things they don’t want to feel, and this I think is really true for a lot of people with eating disorders. So when, after having an argument with her new friend, Eli starts doing vigorous sit-ups, it’s fairly clear this is one of her ways of coping. Another good thing about this show was the depiction of a boy recovering from Anorexia, who seems to act as a source of hope and says things like “feel the fear and do it anyway” when encouraging Eli to eat. Although he does pressure her to eat, saying things like “coward”, which, obviously enough, doesn’t make her suddenly able to eat.
Different ways that families might deal with their daughter/son, sister/brother, etc., having an eating disorder are depicted. For example, Eli’s step-mum takes a picture of Eli’s emancipated body to show her, saying “do you think that’s beautiful?”, and also bakes her a cake with “eat up Ellen” written on it, showing how sometimes people don’t always approach eating disorders in the most tactful way. It’s also clear that she cares a lot for Ellen, organizing for her to see doctors and get inpatient treatment, trying to encourage her to eat. I think this shows how, even when parents/friends/siblings aren’t so helpful, they can still be trying really hard in their own way. So, while this movie is massively triggering for anyone who’s dealt with/is dealing with an eating disorder, it’s also really informative and heartfelt, and real too. That’s why I would recommend, with caution, that people watch this movie and take in what Eli’s going through, but please don’t watch it if you think it will make eating disordered thoughts/behaviors worse.
Mental illness is often glamorized on social media sites like Tumblr. While the site has gotten a lot better for this since I was a teenager, with loads of wonderful blogs encouraging recovery and giving tips for improving self-esteem, there are still some things that worry me. Some content, while not necessarily intending to glamorize mental illness, does perpetuate eating disordered ideas. I’m talking about ‘thinspiration’. This includes images and quotes designed to encourage people to lose weight/not eat, such as “skip dinner, wake up thinner”, as well as pictures of very thin girls/people with severe anorexia, with comments from individuals saying things like “I wish I looked like that”, “so beautiful”,
Tumblr’s tried hard to deal with ‘thinspiration’, for example, a message comes up referring you to helplines if you type in anything to do with thinspiration. Unfortunately, there’s always ways around these things, and thinspiration is still rife under different names (plus you can still continue to content after a warning).
Much of the online ana/mia (anorexia/bulimia) community perpetuates the idea of eating disorders being a ‘lifestyle choice’ and a sign of strength, which is, needless to say, very dangerous. Now, I don’t want to demonize the online eating disorder community; these people are suffering enough. I do want to warn against entering it though. The people who post thinspiration content and ‘eating disorder tips’ are usually very ill and looking for people who understand them, or even just a justification for their behaviors and feelings. The content posted under the veil of mental illness can be damaging to young minds. Some people aren’t able to see that thinspiration is often produced by people feeling intense sadness and fear. This isn’t helped by the fact that non-anorexic ‘thinspiration’ is pretty much everywhere. If you look up healthy lifestyle on Pinterest, you’ll get pictures of skinny women with unrealistically flat stomachs and abs (these woman are probably personal trainers/go to the gym every day), as well as weight loss tips and exercises for a ‘better body’. Obviously, there’s a lot of great body positive stuff out there, but when there’s such an emphasis on being skinny/ ‘ripped’, it shouldn’t be surprising that a lot of young people end up feeling bad about their bodies and can become at risk of getting an eating disorder. So, when there’s also content that explicitly encourages and even gives ‘tips’ for eating disorders it can be really damaging.
It can be difficult for institutions and individuals trying to create content about mental illness without glamorizing it, especially when it comes to movies/TV shows; they need to be entertaining. Not being an expert, I can’t say how to make good content about mental illness, but I think a lot of content makers know that they need to do their research to make a realistic depiction. I also think humor is so, so important; if you’re going to break our hearts at least throw in a joke. It can’t be easy to make media about mental health, so I applaud anyone who does. However, if it becomes glamorizing/triggering, then it might not serve the purpose for which it was intended.
Sometimes mental illness is glamorized as ‘tragically beautiful’, or ‘special’, and I don’t want to disrespect other people’s creativity and/or ways of coping, but I just think it’s untrue to depict mental illness as anything but painful and sucky. So, let’s glamorize health and happiness. Let’s glamorize being able to just eat a chocolate bar without feeling like the world’s ending. Let’s glamorize being able to go out and have a good time with friends, instead of sitting alone in pain. Let’s glamorize strength and resilience. Let’s glamorize recovery.

Eating Disorder relapses: how to prevent and how to cope
A relapse is defined as "a deterioration in someone's state of health after a temporary improvement". In Eating Disorders, this means returning to obsessive thoughts and behaviors around food and weight, negative body image/self-esteem, valuing your weight and/or shape and/or ability to control them more than almost anything else, and returning to damaging behaviors such as restricting, purging and/or binging, as well as obsessive exercise.
Relapses are something to be expected if you're recovering from an eating disorder. You're essentially going from one way of living to a totally new one, where you might have to change your relationship with food, your body, and the entire world around you. Sometimes you might fall back into old habits and feel that you've taken a few massive steps backwards. Sometimes it could be insidious; creeping up on you one missed snack at a time. It can be sorely tempting to ignore the signs and pretend that everything is fine when red flags appear, but it's necessary to be vigilant, especially in the beginning stages of recovery. I know I wouldn't still be recovered if I didn't look out for warnings, no matter how small. So, here's some tips for preventing relapses and coping if you can't:
1. Be vigilant- try to track your mood and eating habits each week, or each day if needed. Are you having at least three meals and two snacks a day? Have you been feeling particularly stressed? If you notice anything worrying, or any negative changes, you can nip problems in the bud by asking for help or using coping skills such as mindfulness (such as focusing on your breaths, counting to 5 as you breathe in an out, and noticing how your body feels), distraction (playing video games, watching television, going for a walk, talking to friends, etc.) and healthy self-talk (such as telling yourself "you are a good person", "you are doing the best you can").
2. Make a plan- having a plan for when problems arise can be so helpful. There's a method called the traffic light method, where you describe a green week, an amber week and a red week in terms of relapse signs. For example, a green week might be one where you stick to your meal plan, talk to your friends and family honestly and manage to avoid any unhealthy coping mechanisms. An amber week might be one where you're finding it harder to be honest with your friends, maybe you don't feel like going out as much, and you might skip a meal or two, or find yourself more anxious about calories/food/weight, but you are still broadly managing to cope, although things might be more of a struggle. A red week might involve returning to unhealthy coping mechanisms such as purging, not eating very well, where your mood is lower/more anxious and you might start lying to people around you. However your plan looks is great, as long as it makes sense to you and will help you keep track of where you're at in terms of recovery. If you've struggled with Anorexia Nervosa and/or being underweight it might also be necessary to add weight loss to your list of warning signs. If you still need to gain weight then no weight gain might be part of an amber week, and weight loss might be a red week.
3. Have a support system- make sure that the people around you are aware of your relapse signs and how you want them to help you. You might want them to gently prompt you to eat healthier or talk to them, you might just want them to acknowledge that you're struggling and let you know their there. You might think it's necessary for them to get more involved in your eating, or you might just want them in the background. However you want them to help you, having a support system around you is so vital to staying healthy. If you don't feel like you have a support system around you, it might be helpful to go to a local group of some kind, such as a creative writing group, art group or reading club. If this is particularly difficult it might help to see a therapist or counselor for advice and support.
4. Don't confuse a lapse for a relapse- it can be really difficult if we experience a blip to not label it as a relapse. If there's an episode of purging we might think we're back to square one, or if we don't eat properly for a day we might think we've blown it. That's just not true. A relapse is being right back to square one, where we were before recovery, or dangerously close to it. A blip is struggling and possibly engaging in old, unhealthy behaviors, in the very short term. If you find yourself binging and/or purging/not eating/restricting, this doesn't necessarily mean you've had a relapse. It may be that you're struggling and need to seriously think about using more coping strategies and intensive skills you've learned throughout treatment. For example, if during treatment you learnt that you need to eat three meals and three snacks a day, but over the last couple of days you've only had one/two meals, then try to make sure you have three meals and three snacks. Consider having someone sit with you while you eat and recording you're intake to make sure you're having enough. Just because you find yourself needing to more intensively use coping strategies, and find yourself struggling, doesn't mean you've gone back to the start. If it's a blip them you're still able to recognize that there's a problem, and try to use coping skills. In a blip you'll be struggling, sure, but you won't be constantly behaving like you used to. If you label a blip as a relapse it can be really disheartening and can actually make you feel less motivated to stay healthy, and more likely to actually have a full relapse and become ill again. Give yourself the benefit of the doubt and just keep trying.
5. Don't beat yourself up- it can be very easy to get angry at yourself or blame yourself if you start to struggle/engage in old behaviors. But practicing self-compassion is so important, and we all deserve it. This is part of a therapy called Compassion Focused Therapy (CFT), which involves cultivating our 'compassion system', which involves self-soothing (the ability to calm ourselves down and make ourselves feel better) and self-acceptance. One task in CFT is to create your 'compassionate self', which can be based on a real person/real people, or someone fictional. It should be a character who is kind to you, understanding and gives you what you need, which you can incorporate into yourself and call upon when things get difficult. It may say things like "I understand that you're struggling right now, but you'll be okay".
6. Get help- don't struggle alone. You really don't need to. There's lots of help out there, whether it's from your own family/friends, online, or your GP/therapist. There is someone out there who will listen to you and try to help. It's a difficult, but also incredibly brave thing, to reach out and admit that you're struggling. Whether it's a blip or a relapse, if you feel like you want/need help, then you should get it. Everyone needs support sometimes, and if you've struggled with an eating disorder then it's likely you'll need it too. If you're engaging in destructive behaviors like not eating enough, making yourself sick/using laxatives, binging or self-harm, and/or you've lost a lot of weight in a short amount of time, then you should see your GP as soon as possible.
Remember, Eating Disorders don't just go away over night, and sometimes they can crawl their way back into our minds. We just have to be vigilant and tough, and make sure they don't stay.
Above all I think it's really important to not give up hope, as cheesy and annoying as that sounds. Stephen Hawking said "While there is life, there is hope", and we must do our best to remember that, even when it's difficult.
Some helpful resources:
https://www.beateatingdisorders.org.uk/your-stories/recovery/recognising-relapse-personal-perspective
https://www.beateatingdisorders.org.uk/
https://www.nationaleatingdisorders.org/blog/10-ways-cope-with-relapse-eating-disorder-recovery
A relapse is defined as "a deterioration in someone's state of health after a temporary improvement". In Eating Disorders, this means returning to obsessive thoughts and behaviors around food and weight, negative body image/self-esteem, valuing your weight and/or shape and/or ability to control them more than almost anything else, and returning to damaging behaviors such as restricting, purging and/or binging, as well as obsessive exercise.
Relapses are something to be expected if you're recovering from an eating disorder. You're essentially going from one way of living to a totally new one, where you might have to change your relationship with food, your body, and the entire world around you. Sometimes you might fall back into old habits and feel that you've taken a few massive steps backwards. Sometimes it could be insidious; creeping up on you one missed snack at a time. It can be sorely tempting to ignore the signs and pretend that everything is fine when red flags appear, but it's necessary to be vigilant, especially in the beginning stages of recovery. I know I wouldn't still be recovered if I didn't look out for warnings, no matter how small. So, here's some tips for preventing relapses and coping if you can't:
1. Be vigilant- try to track your mood and eating habits each week, or each day if needed. Are you having at least three meals and two snacks a day? Have you been feeling particularly stressed? If you notice anything worrying, or any negative changes, you can nip problems in the bud by asking for help or using coping skills such as mindfulness (such as focusing on your breaths, counting to 5 as you breathe in an out, and noticing how your body feels), distraction (playing video games, watching television, going for a walk, talking to friends, etc.) and healthy self-talk (such as telling yourself "you are a good person", "you are doing the best you can").
2. Make a plan- having a plan for when problems arise can be so helpful. There's a method called the traffic light method, where you describe a green week, an amber week and a red week in terms of relapse signs. For example, a green week might be one where you stick to your meal plan, talk to your friends and family honestly and manage to avoid any unhealthy coping mechanisms. An amber week might be one where you're finding it harder to be honest with your friends, maybe you don't feel like going out as much, and you might skip a meal or two, or find yourself more anxious about calories/food/weight, but you are still broadly managing to cope, although things might be more of a struggle. A red week might involve returning to unhealthy coping mechanisms such as purging, not eating very well, where your mood is lower/more anxious and you might start lying to people around you. However your plan looks is great, as long as it makes sense to you and will help you keep track of where you're at in terms of recovery. If you've struggled with Anorexia Nervosa and/or being underweight it might also be necessary to add weight loss to your list of warning signs. If you still need to gain weight then no weight gain might be part of an amber week, and weight loss might be a red week.
3. Have a support system- make sure that the people around you are aware of your relapse signs and how you want them to help you. You might want them to gently prompt you to eat healthier or talk to them, you might just want them to acknowledge that you're struggling and let you know their there. You might think it's necessary for them to get more involved in your eating, or you might just want them in the background. However you want them to help you, having a support system around you is so vital to staying healthy. If you don't feel like you have a support system around you, it might be helpful to go to a local group of some kind, such as a creative writing group, art group or reading club. If this is particularly difficult it might help to see a therapist or counselor for advice and support.
4. Don't confuse a lapse for a relapse- it can be really difficult if we experience a blip to not label it as a relapse. If there's an episode of purging we might think we're back to square one, or if we don't eat properly for a day we might think we've blown it. That's just not true. A relapse is being right back to square one, where we were before recovery, or dangerously close to it. A blip is struggling and possibly engaging in old, unhealthy behaviors, in the very short term. If you find yourself binging and/or purging/not eating/restricting, this doesn't necessarily mean you've had a relapse. It may be that you're struggling and need to seriously think about using more coping strategies and intensive skills you've learned throughout treatment. For example, if during treatment you learnt that you need to eat three meals and three snacks a day, but over the last couple of days you've only had one/two meals, then try to make sure you have three meals and three snacks. Consider having someone sit with you while you eat and recording you're intake to make sure you're having enough. Just because you find yourself needing to more intensively use coping strategies, and find yourself struggling, doesn't mean you've gone back to the start. If it's a blip them you're still able to recognize that there's a problem, and try to use coping skills. In a blip you'll be struggling, sure, but you won't be constantly behaving like you used to. If you label a blip as a relapse it can be really disheartening and can actually make you feel less motivated to stay healthy, and more likely to actually have a full relapse and become ill again. Give yourself the benefit of the doubt and just keep trying.
5. Don't beat yourself up- it can be very easy to get angry at yourself or blame yourself if you start to struggle/engage in old behaviors. But practicing self-compassion is so important, and we all deserve it. This is part of a therapy called Compassion Focused Therapy (CFT), which involves cultivating our 'compassion system', which involves self-soothing (the ability to calm ourselves down and make ourselves feel better) and self-acceptance. One task in CFT is to create your 'compassionate self', which can be based on a real person/real people, or someone fictional. It should be a character who is kind to you, understanding and gives you what you need, which you can incorporate into yourself and call upon when things get difficult. It may say things like "I understand that you're struggling right now, but you'll be okay".
6. Get help- don't struggle alone. You really don't need to. There's lots of help out there, whether it's from your own family/friends, online, or your GP/therapist. There is someone out there who will listen to you and try to help. It's a difficult, but also incredibly brave thing, to reach out and admit that you're struggling. Whether it's a blip or a relapse, if you feel like you want/need help, then you should get it. Everyone needs support sometimes, and if you've struggled with an eating disorder then it's likely you'll need it too. If you're engaging in destructive behaviors like not eating enough, making yourself sick/using laxatives, binging or self-harm, and/or you've lost a lot of weight in a short amount of time, then you should see your GP as soon as possible.
Remember, Eating Disorders don't just go away over night, and sometimes they can crawl their way back into our minds. We just have to be vigilant and tough, and make sure they don't stay.
Above all I think it's really important to not give up hope, as cheesy and annoying as that sounds. Stephen Hawking said "While there is life, there is hope", and we must do our best to remember that, even when it's difficult.
Some helpful resources:
https://www.beateatingdisorders.org.uk/your-stories/recovery/recognising-relapse-personal-perspective
https://www.beateatingdisorders.org.uk/
https://www.nationaleatingdisorders.org/blog/10-ways-cope-with-relapse-eating-disorder-recovery

News, the Internet and Mental Health
When I type in ‘meditation’ to YouTube, ‘meditation for anxiety’ is the 5th response. ‘Why am I’ yields the responses ‘so tired’ and ‘so depressed’ when typed into Google. ‘Why are millennials’ yields the responses ‘so sad’, ‘so needy’ and ‘so weak’. Basically, although this is no scientific test, I think it’s reasonable to conclude that a lot of people, especially in my generation, are feeling stressed out. There are many reasons why this may be; perhaps mental health issues are simply more recognised and diagnosed nowadays. Perhaps it’s all that dang TV we watched as children, or the smart-phone world we live in. Maybe social media really is creating a vacuum of self-indulgence and self-hatred. There are a lot of things that could have led to the increase in stress and anxiety over the last few decades; an increase in social media use, twenty-four-hour rolling news, a broken housing market and economic problems, and that’s just off the top of my head.
The thing is, all generations have multiple, difficult to deal with stressors; nuclear war in the 60’s, aids in the 80’s, Y2K in the late 90’s, terrorism in the noughties, etc. Now, though, we’re constantly exposed to all of the worlds problems, and it’s never ending. We get the news all day on the television and internet. We get beeping notifications for breaking news, which seems nearly constant. I’m not saying news is bad; it’s obviously necessary and good to know what’s going on with the world. However, the issue with constant news is that it can bombard your mind with worrying information and images that you can’t do anything about and can make you feel helpless (see Adam Curtis’s ‘Oh Dearism’ on YouTube).
If you have anxiety anyway, then news is probably not going to help. My suggestion would be not to completely boycott the news, but to discover your own limits and stick to them. One way to do this is to monitor what you’re watching and your moods throughout the day, and then to find any correlations between news/internet/television exposure and anxiety/low mood. Basically, does watching the news everyday make you anxious, or make your mood negative? If so, you should probably avoid it for a little while. Do you feel better if you only check the news once a week? Do that! It sounds simpler than it is, I know, but it really is beneficial to figure out if your being stressed out by the news, because, although anxiety can come out of nowhere, it can also be triggered by external inputs, and these can be controlled. It is not selfish to want to distance yourself from the worlds events; for the most part you cannot do anything about them anyway.
Now, once we’ve dealt with any anxiety/low mood the news might be causing, we might want to turn to the internet in general. Social media can also be anxiety provoking; studies have shown that teenage girls who spend more time on social media, and who alter their photographs, are much more likely to show eating-disorder attitudes and food problems. Of course, it is totally possible that people with predispositions to eating problems are simply more likely to go on social media and alter their photographs, but from my own experience I know that, even if you seek out social media and the like because you already have issues, they can make said issues worse. It’s helpful to set yourself some rules if you’re struggling with mental health issues, or even if you just want to avoid negativity in your life, so here’s some suggestions from me and my girlfriend:
Please also remember that it is not selfish to put yourself first; if you listen to your intuition, without worrying about what other’s might think or what you ‘have’ to do, then you’ll probably realise you already know exactly what you need.
When I type in ‘meditation’ to YouTube, ‘meditation for anxiety’ is the 5th response. ‘Why am I’ yields the responses ‘so tired’ and ‘so depressed’ when typed into Google. ‘Why are millennials’ yields the responses ‘so sad’, ‘so needy’ and ‘so weak’. Basically, although this is no scientific test, I think it’s reasonable to conclude that a lot of people, especially in my generation, are feeling stressed out. There are many reasons why this may be; perhaps mental health issues are simply more recognised and diagnosed nowadays. Perhaps it’s all that dang TV we watched as children, or the smart-phone world we live in. Maybe social media really is creating a vacuum of self-indulgence and self-hatred. There are a lot of things that could have led to the increase in stress and anxiety over the last few decades; an increase in social media use, twenty-four-hour rolling news, a broken housing market and economic problems, and that’s just off the top of my head.
The thing is, all generations have multiple, difficult to deal with stressors; nuclear war in the 60’s, aids in the 80’s, Y2K in the late 90’s, terrorism in the noughties, etc. Now, though, we’re constantly exposed to all of the worlds problems, and it’s never ending. We get the news all day on the television and internet. We get beeping notifications for breaking news, which seems nearly constant. I’m not saying news is bad; it’s obviously necessary and good to know what’s going on with the world. However, the issue with constant news is that it can bombard your mind with worrying information and images that you can’t do anything about and can make you feel helpless (see Adam Curtis’s ‘Oh Dearism’ on YouTube).
If you have anxiety anyway, then news is probably not going to help. My suggestion would be not to completely boycott the news, but to discover your own limits and stick to them. One way to do this is to monitor what you’re watching and your moods throughout the day, and then to find any correlations between news/internet/television exposure and anxiety/low mood. Basically, does watching the news everyday make you anxious, or make your mood negative? If so, you should probably avoid it for a little while. Do you feel better if you only check the news once a week? Do that! It sounds simpler than it is, I know, but it really is beneficial to figure out if your being stressed out by the news, because, although anxiety can come out of nowhere, it can also be triggered by external inputs, and these can be controlled. It is not selfish to want to distance yourself from the worlds events; for the most part you cannot do anything about them anyway.
Now, once we’ve dealt with any anxiety/low mood the news might be causing, we might want to turn to the internet in general. Social media can also be anxiety provoking; studies have shown that teenage girls who spend more time on social media, and who alter their photographs, are much more likely to show eating-disorder attitudes and food problems. Of course, it is totally possible that people with predispositions to eating problems are simply more likely to go on social media and alter their photographs, but from my own experience I know that, even if you seek out social media and the like because you already have issues, they can make said issues worse. It’s helpful to set yourself some rules if you’re struggling with mental health issues, or even if you just want to avoid negativity in your life, so here’s some suggestions from me and my girlfriend:
- Don’t set news notifications; if you want the news you can get it, but if it comes to you, you can’t avoid it.
- DO NOT go on any pro-ana/pro-mia sites, EVER!
- Time limits can be really helpful, for example, two hours at a time, and then giving yourself a break.
- Remember social media shows the highlights of other people’s lives, not the truth, don’t compare yourself to the enhanced reflections of others online.
- Look out for good things that are happening in the world; even if you’re just watching Russell Howard’s good news. I also found this lovely website filled with purely good news: https://www.goodnewsnetwork.org/
- If messaging stresses you out, it’s okay to leave your phone for a while, even if you need to explain to friends and family that you can’t always get back to them right away. If that beeping from your phone is making your heart race, turn it off. It’s okay.
Please also remember that it is not selfish to put yourself first; if you listen to your intuition, without worrying about what other’s might think or what you ‘have’ to do, then you’ll probably realise you already know exactly what you need.
Mental Health stigma: violence
Did you know that people with schizophrenia are more likely to be hurt by someone, or to hurt themselves, than to hurt someone else? Did you also know that most forms of mental illness are incapacitating? Meaning that people are too ill to be able to plan a crime or to hurt anyone, even if they wanted to. In fact, according to Mental Health Statistics, mental health and behavioural problems are a primary cause of disability worldwide, causing over 40 million years of disability in 20 to 29-year-olds. So, while around 70% of prisoners have two or more mental illnesses (making mental illness more prevalent in prison than the general population), that doesn’t mean people with mental illness are more dangerous than other people.
There is some stigma surrounding the idea that people with mental health problems are ‘dangerous’, so I wanted to present some facts from Mental Health Statistics:
• More than 90% of suicides and suicide attempts have been associated with a psychiatric disorder.
• People with severe mental health problems are much more likely to harm themselves than others; in 2013, there were 1876 recorded suicides among mental health inpatients, and only 51 homicides.
• In 2013 a survey of people with severe mental health problems found that 45% had been victims of a crime in the past year, one in five have experienced a violent assault and people with mental health problems were five times more likely to be a victim of assault than those without, with women who had severe mental health problems being 10 times more likely.
These startling facts show something vitally important; people with mental health issues are not dangerous, and are in fact, in danger from themselves and others. So, why does the idea that people with certain mental illness are dangerous endure? Well, there’s movies like Psycho, The Roommate, and Split, which, while good movies and all, do depict mentally ill people as dangerous, so probably don’t help. What I think the biggest issue is, though, is that people aren’t taught about mental health that much, and humans have a natural tendency to fear that which they are unfamiliar with. Not realising that your parents, your child, your best friend or that nice man who smiled at you on the bus has dealt with mental illness can make people feel like it’s not relevant to them and can make people rely on scary news articles like ‘Flinders Street rampage accused diagnosed with paranoid schizophrenia’ and ‘Man with schizophrenia may be released after three years’ for their knowledge of mental health. The news has a generally negative bias, and so it shouldn’t be surprising that a lot of the news around mental health revolves around people with psychiatric problems committing crimes, especially those who suffer from psychotic illnesses.
I don’t want to overlook all of the good work people have been doing to raise awareness for mental health issues, from positive representations of mental health recovery in documentaries such as The Secret Life of A Manic Depressive by Stephen Fry (free on YouTube, hint hint) and the genuinely moving advert from Lloyds Bank about mental health labels. Great things are being done and will continue to be done in order to raise awareness and help people who are struggling, and that is amazing. There was a time when people with anxiety disorders were taken to asylums for their entire lives and given electro-shock therapy. I’d have been screwed in the 1950’s. We do live in a rather positive time for mental health care and awareness.
On the other hand, I think it’s important for stigma to be addressed and the reality of mental health to be understood. Mental health disorders can involve isolation, self-harm, self-destructive behaviour, emotional turmoil, confusion, despair, not washing or brushing your hair for a week because you just can’t, masking how you feel, pushing people away. People with ‘scary’ illness like psychosis do not just ‘see things’ or hear voices, they suffer from an array of dissociative experiences, including, among hallucinations, a feeling of being outside of one’s own body, low mood/inappropriate emotions, an inability to care for oneself, impaired motor functions, thought disorder (loose associations, such as associating door with wood and changing the conversation to trees), and many more. While a lot of representation of mental illness such as psychosis involve the tiny minority of those who commit violent crimes, most people with psychosis are extremely vulnerable, unable to work and at risk of assault themselves. If the only representation of flowers we had were Venus Flytraps, we’d be scared of daisies.
So, please don’t be scared of people with mental illnesses, or of talking about mental health.
References:
https://www.mentalhealth.org.uk/publications/fundamental-facts-about-mental-health-2016
Did you know that people with schizophrenia are more likely to be hurt by someone, or to hurt themselves, than to hurt someone else? Did you also know that most forms of mental illness are incapacitating? Meaning that people are too ill to be able to plan a crime or to hurt anyone, even if they wanted to. In fact, according to Mental Health Statistics, mental health and behavioural problems are a primary cause of disability worldwide, causing over 40 million years of disability in 20 to 29-year-olds. So, while around 70% of prisoners have two or more mental illnesses (making mental illness more prevalent in prison than the general population), that doesn’t mean people with mental illness are more dangerous than other people.
There is some stigma surrounding the idea that people with mental health problems are ‘dangerous’, so I wanted to present some facts from Mental Health Statistics:
• More than 90% of suicides and suicide attempts have been associated with a psychiatric disorder.
• People with severe mental health problems are much more likely to harm themselves than others; in 2013, there were 1876 recorded suicides among mental health inpatients, and only 51 homicides.
• In 2013 a survey of people with severe mental health problems found that 45% had been victims of a crime in the past year, one in five have experienced a violent assault and people with mental health problems were five times more likely to be a victim of assault than those without, with women who had severe mental health problems being 10 times more likely.
These startling facts show something vitally important; people with mental health issues are not dangerous, and are in fact, in danger from themselves and others. So, why does the idea that people with certain mental illness are dangerous endure? Well, there’s movies like Psycho, The Roommate, and Split, which, while good movies and all, do depict mentally ill people as dangerous, so probably don’t help. What I think the biggest issue is, though, is that people aren’t taught about mental health that much, and humans have a natural tendency to fear that which they are unfamiliar with. Not realising that your parents, your child, your best friend or that nice man who smiled at you on the bus has dealt with mental illness can make people feel like it’s not relevant to them and can make people rely on scary news articles like ‘Flinders Street rampage accused diagnosed with paranoid schizophrenia’ and ‘Man with schizophrenia may be released after three years’ for their knowledge of mental health. The news has a generally negative bias, and so it shouldn’t be surprising that a lot of the news around mental health revolves around people with psychiatric problems committing crimes, especially those who suffer from psychotic illnesses.
I don’t want to overlook all of the good work people have been doing to raise awareness for mental health issues, from positive representations of mental health recovery in documentaries such as The Secret Life of A Manic Depressive by Stephen Fry (free on YouTube, hint hint) and the genuinely moving advert from Lloyds Bank about mental health labels. Great things are being done and will continue to be done in order to raise awareness and help people who are struggling, and that is amazing. There was a time when people with anxiety disorders were taken to asylums for their entire lives and given electro-shock therapy. I’d have been screwed in the 1950’s. We do live in a rather positive time for mental health care and awareness.
On the other hand, I think it’s important for stigma to be addressed and the reality of mental health to be understood. Mental health disorders can involve isolation, self-harm, self-destructive behaviour, emotional turmoil, confusion, despair, not washing or brushing your hair for a week because you just can’t, masking how you feel, pushing people away. People with ‘scary’ illness like psychosis do not just ‘see things’ or hear voices, they suffer from an array of dissociative experiences, including, among hallucinations, a feeling of being outside of one’s own body, low mood/inappropriate emotions, an inability to care for oneself, impaired motor functions, thought disorder (loose associations, such as associating door with wood and changing the conversation to trees), and many more. While a lot of representation of mental illness such as psychosis involve the tiny minority of those who commit violent crimes, most people with psychosis are extremely vulnerable, unable to work and at risk of assault themselves. If the only representation of flowers we had were Venus Flytraps, we’d be scared of daisies.
So, please don’t be scared of people with mental illnesses, or of talking about mental health.
References:
https://www.mentalhealth.org.uk/publications/fundamental-facts-about-mental-health-2016
What is an anxiety disorder?
Ahh, anxiety, the worst public speaker in the world. The epitome of preparing for the worst. We all feel anxiety sometimes, but we, obviously, do not all have an anxiety disorder. So, what is an anxiety disorder anyway? How is it different from regular old anxiety? Well, anxiety is the complicated cocktail of emotions consisting of apprehension about the future, thoughts such as 'things are going to go wrong' and feelings such as butterflies in the stomach. Anxiety is most likely an evolved mechanism which allows humans to prepare for future threats and be ready for the fight-or-flight reaction involved in fear (which occurs when we are/feel we are in immediate danger and our hearts beat very fast, we might get sweaty, feel like we want to run, etc.). Anxiety can occur when we are concerned about a future event, and it is very normal. However, when anxiety is out of proportion to any actual danger, when it interferes with daily life, leads to an inability to function/severe and persistent distress, then it's an anxiety disorder.
To help illustrate this let me tell you two stories:
Fiona is 21, she's nervous because she has a big presentation at work tomorrow and she's worried that she might embarrass herself/it might go wrong. She has butterflies in her stomach and feels a little bit shaky, but she works on her presentation in front of the mirror and manages to go to work and do it. Fiona is anxious.
Joanna is 21, she is nervous because she had an intrusive thought about abuse and is worried that she is a terrible person. She is also concerned because her heart is racing and she fears she might have a heart attack. She feels very sick and is often very tired. Joanna does not go into work because she feels unwell and unable to cope with seeing people. Joanna has missed work before and is worried that she might get fired. She has been unable to sleep although she is tired and her breathing is shallow and difficult. Joanna has an anxiety disorder.
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) someone can be diagnosed with an anxiety disorder if they have experienced persistent and debilitating/distressing anxiety for at least six months, and it must be clearly excessive. Joanna's worries are clearly excessive, and some of them are also irrational (e.g. worrying about having a heart attack/being a bad person), so she has an anxiety disorder. Some anxiety disorders, such as generalised anxiety disorder (GAD), can involve worries and anxiety that come out of the blue, seemingly for no reason. Some people experience increased anxiety symptoms during times of stress, whereas other people experience anxiety at 'random' times. People with anxiety disorders can present very differently, and there are many types of disorder in this category, so here's a list:
1. Generalized anxiety disorder (GAD).
2. Obsessive compulsive disorder (OCD).
3. Panic disorder (with or without agoraphobia).
4. Social phobia.
5. Specific phobia.
6. Post-traumatic stress disorder (PTSD).
As you can see, there are many different types of anxiety disorder. I will just outline a couple for today: OCD and GAD.
OCD has recently been given it's own category by the DSM-V, so isn't technically considered an anxiety disorder, but due to it's commonalities with anxiety disorders is it often grouped with them. OCD involves obsessions and compulsions. Obsessions are unwanted and intense images, thoughts and/or urges. Compulsions are ritualistic behaviors performed to minimise anxiety caused by obsessions/stop something bad from happening. Obsessions come in four main types: Contamination/illness, harm, religious/sexual and symmetry/order, and can be paired with compulsions such as cleaning excessively, checking behaviors (e.g. checking that the stove is off multiple times before leaving the house), mental rituals (e.g. repeating a calming phrase in one's head or praying) and organizing/re-organizing things many times. OCD can only be diagnosed if compulsions/obsessions take at least an hour out of a persons day. While, contrary to popular belief, OCD can exist without compulsions, 90% of people with obsessions also have compulsions, and this figure goes up to 98% when mental compulsions are included. It is not clear why people get OCD, but several theories exist to explain it's development. For example, some psychologists believe that an increased feeling of responsibility is a factor in the disorder, causing people to feel responsible for their own thoughts. Similarly, thought-action-fusion, where people believe thoughts can increase the probability of something happening, or thinking about something is morally the same as doing it, may also be important. For example, someone may think about their mother having a car crash and then worry that this event is now more likely because they thought about it. They may then engage in a compulsion such as praying in an attempt to stop this from happening. One thing that is certain is that OCD can be a very debilitating illness which often causes severe distress. Treatments are available, from CBT to exposure therapy and medication, and the good news is most people can recover.
GAD is basically worrying all the time. I can't really explain it any better. I can't speak for everyone with the disorder, but for me at least (having at least symptoms of it) it's kind of like having a radio in your head that you can't turn off, and it's constantly telling you bad news. It's like constantly having a feeling that something is wrong, but not being able to explain it. More scientifically, symptoms of GAD include excessive worry about multiple areas of life, such as health, loved ones, work, school, etc. People with GAD often also have physical symptoms such as restlessness, sickness, bowel problems, trouble sleeping and others. People with GAD do not need to have panic attacks for a diagnosis, but they may get panic attacks sometimes. Panic attacks involve intense feelings of fear, nausea, shakiness, trouble breathing, racing heart, sweating, fear of dying or going insane, and are very, very scary. In fact, over half of those with an anxiety disorder go to emergency rooms with panic attacks because they feel that they could only feel like that if they were dying. Treatments for this disorder include Selective Serotonin Re-uptake Inhibitors (SSRI's), also known as anti-depressants, CBT and other talking therapies. Anxiolytics (anti-anxiety drugs) can be used, but Benzodiazapines, due to their dangerous side effects, are not recommended.
Anxiety disorders are very scary, and they can cause much more than just fear. They can cause guilt about being anxious all the time and putting strain on loved ones. They can cause worrying about worrying. They can cause self-doubt and sadness, even depression. Basically, they suck. If you're dealing with an anxiety disorder or symptoms of one, don't lose hope, it is, believe it or not, manageable. If you think you might have an anxiety disorder then go to your GP. They will most likely give you questionnaires and other tests, such as the Beck Anxiety Inventory, which will inform them if you have an anxiety disorder and how severe it is. They will also probably refer you to specialist psychologists/psychiatrists who can give you a more in-depth assessment and come up with a treatment plan that you agree to. Any treatments offered are, of course, optional, and if you feel that one treatment isn't working for you, you can always try another.
Here are some helpful links:
https://www.verywellmind.com/dsm-5-criteria-for-generalized-anxiety-disorder-1393147
https://www.mind.org.uk/information-support/types-of-mental-health-problems/anxiety-and-panic-attacks/anxiety-disorders/
Ahh, anxiety, the worst public speaker in the world. The epitome of preparing for the worst. We all feel anxiety sometimes, but we, obviously, do not all have an anxiety disorder. So, what is an anxiety disorder anyway? How is it different from regular old anxiety? Well, anxiety is the complicated cocktail of emotions consisting of apprehension about the future, thoughts such as 'things are going to go wrong' and feelings such as butterflies in the stomach. Anxiety is most likely an evolved mechanism which allows humans to prepare for future threats and be ready for the fight-or-flight reaction involved in fear (which occurs when we are/feel we are in immediate danger and our hearts beat very fast, we might get sweaty, feel like we want to run, etc.). Anxiety can occur when we are concerned about a future event, and it is very normal. However, when anxiety is out of proportion to any actual danger, when it interferes with daily life, leads to an inability to function/severe and persistent distress, then it's an anxiety disorder.
To help illustrate this let me tell you two stories:
Fiona is 21, she's nervous because she has a big presentation at work tomorrow and she's worried that she might embarrass herself/it might go wrong. She has butterflies in her stomach and feels a little bit shaky, but she works on her presentation in front of the mirror and manages to go to work and do it. Fiona is anxious.
Joanna is 21, she is nervous because she had an intrusive thought about abuse and is worried that she is a terrible person. She is also concerned because her heart is racing and she fears she might have a heart attack. She feels very sick and is often very tired. Joanna does not go into work because she feels unwell and unable to cope with seeing people. Joanna has missed work before and is worried that she might get fired. She has been unable to sleep although she is tired and her breathing is shallow and difficult. Joanna has an anxiety disorder.
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) someone can be diagnosed with an anxiety disorder if they have experienced persistent and debilitating/distressing anxiety for at least six months, and it must be clearly excessive. Joanna's worries are clearly excessive, and some of them are also irrational (e.g. worrying about having a heart attack/being a bad person), so she has an anxiety disorder. Some anxiety disorders, such as generalised anxiety disorder (GAD), can involve worries and anxiety that come out of the blue, seemingly for no reason. Some people experience increased anxiety symptoms during times of stress, whereas other people experience anxiety at 'random' times. People with anxiety disorders can present very differently, and there are many types of disorder in this category, so here's a list:
1. Generalized anxiety disorder (GAD).
2. Obsessive compulsive disorder (OCD).
3. Panic disorder (with or without agoraphobia).
4. Social phobia.
5. Specific phobia.
6. Post-traumatic stress disorder (PTSD).
As you can see, there are many different types of anxiety disorder. I will just outline a couple for today: OCD and GAD.
OCD has recently been given it's own category by the DSM-V, so isn't technically considered an anxiety disorder, but due to it's commonalities with anxiety disorders is it often grouped with them. OCD involves obsessions and compulsions. Obsessions are unwanted and intense images, thoughts and/or urges. Compulsions are ritualistic behaviors performed to minimise anxiety caused by obsessions/stop something bad from happening. Obsessions come in four main types: Contamination/illness, harm, religious/sexual and symmetry/order, and can be paired with compulsions such as cleaning excessively, checking behaviors (e.g. checking that the stove is off multiple times before leaving the house), mental rituals (e.g. repeating a calming phrase in one's head or praying) and organizing/re-organizing things many times. OCD can only be diagnosed if compulsions/obsessions take at least an hour out of a persons day. While, contrary to popular belief, OCD can exist without compulsions, 90% of people with obsessions also have compulsions, and this figure goes up to 98% when mental compulsions are included. It is not clear why people get OCD, but several theories exist to explain it's development. For example, some psychologists believe that an increased feeling of responsibility is a factor in the disorder, causing people to feel responsible for their own thoughts. Similarly, thought-action-fusion, where people believe thoughts can increase the probability of something happening, or thinking about something is morally the same as doing it, may also be important. For example, someone may think about their mother having a car crash and then worry that this event is now more likely because they thought about it. They may then engage in a compulsion such as praying in an attempt to stop this from happening. One thing that is certain is that OCD can be a very debilitating illness which often causes severe distress. Treatments are available, from CBT to exposure therapy and medication, and the good news is most people can recover.
GAD is basically worrying all the time. I can't really explain it any better. I can't speak for everyone with the disorder, but for me at least (having at least symptoms of it) it's kind of like having a radio in your head that you can't turn off, and it's constantly telling you bad news. It's like constantly having a feeling that something is wrong, but not being able to explain it. More scientifically, symptoms of GAD include excessive worry about multiple areas of life, such as health, loved ones, work, school, etc. People with GAD often also have physical symptoms such as restlessness, sickness, bowel problems, trouble sleeping and others. People with GAD do not need to have panic attacks for a diagnosis, but they may get panic attacks sometimes. Panic attacks involve intense feelings of fear, nausea, shakiness, trouble breathing, racing heart, sweating, fear of dying or going insane, and are very, very scary. In fact, over half of those with an anxiety disorder go to emergency rooms with panic attacks because they feel that they could only feel like that if they were dying. Treatments for this disorder include Selective Serotonin Re-uptake Inhibitors (SSRI's), also known as anti-depressants, CBT and other talking therapies. Anxiolytics (anti-anxiety drugs) can be used, but Benzodiazapines, due to their dangerous side effects, are not recommended.
Anxiety disorders are very scary, and they can cause much more than just fear. They can cause guilt about being anxious all the time and putting strain on loved ones. They can cause worrying about worrying. They can cause self-doubt and sadness, even depression. Basically, they suck. If you're dealing with an anxiety disorder or symptoms of one, don't lose hope, it is, believe it or not, manageable. If you think you might have an anxiety disorder then go to your GP. They will most likely give you questionnaires and other tests, such as the Beck Anxiety Inventory, which will inform them if you have an anxiety disorder and how severe it is. They will also probably refer you to specialist psychologists/psychiatrists who can give you a more in-depth assessment and come up with a treatment plan that you agree to. Any treatments offered are, of course, optional, and if you feel that one treatment isn't working for you, you can always try another.
Here are some helpful links:
https://www.verywellmind.com/dsm-5-criteria-for-generalized-anxiety-disorder-1393147
https://www.mind.org.uk/information-support/types-of-mental-health-problems/anxiety-and-panic-attacks/anxiety-disorders/
Explaining self-harm scars to children
Self-harm scars can be difficult enough to explain to adults, but if there’s a child in your life asking about them it can be overwhelming trying to figure out how to talk to them. There are several options for dealing with this predicament, which I will outline below:
1. Make something up- this is often a go-to for people who really don’t know what to say to someone asking them about self-harm. It’s often an automatic fear response, because telling anyone that you intentionally hurt yourself is difficult but trying to explain the complex reasons behind self-harm, and what it is in the first place, to a child, might seem far too difficult. This option is one which I do not discourage, especially if you’re just not ready to speak about it. You don’t owe anyone an explanation from your scars, even your own children or family members.
2. Explain it- this is a difficult one, but I think it’s worthwhile, particularly if you are being asked about scars by your own children/a sibling/family member you see a lot/are close to. Depending on the age-group, there are different ways of explaining self-harm. For younger children, I would recommend saying something along the lines of ‘just like people get sick in their bodies, you can also get sick in your brain, and that’s what gave me scars’, additionally, if you have recovered I would recommend adding the comforting sentence ‘but I’m doing better now’. Usually younger children won’t ask further questions, and it’s not necessary to get into all the details. Being as calm as possible and speaking in an age-appropriate but frank way will usually ensure that a child feels their questions have been answered. Older children might be ready to hear more about mental illness, and so it might be a good idea to have a longer conversation with them about how emotions and thoughts can lead to problems, including self-harm. What is important to remember is that self-harm is nothing to be ashamed of, and neither is mental illness, speaking openly and honestly to your children about mental health and your own experiences can actually be beneficial in encouraging children and young adults to speak about their own problems, and it makes it more likely that they will go to you in the future if they are struggling.
3. Tell their parents- if the child is not your own then you might consider talking to their parents about your self-harm scars. If you politely mention that their child has asked about the scars, and explain the situation, you can leave the decision of whether or not to explain it to their child to the parents. Some parents may want their children to be informed, whereas others might not think it appropriate to tell their children about self-harm until they are older. For this reason, I feel it is more respectful to ask a parent how they want to handle the situation than to tell the child about it yourself.
Given that we are on the topic of self-harm scars, another important thing to note is that showing self-harm scars is alright. If you chose to wear clothing that shows your scars that’s your decision and you do not need to explain yourself to anyone. On the other hand, showing fresh wounds may be a different matter. One issue with showing wounds is that these can be distressing as they are clearly recent injuries. On the other hand, on a hot day you should not have to overheat because of your self-harm. At the end of the day, what you should be focusing on is recovery and staying safe, not what others might think or worries about how to explain scars. If you have the same worry I do, that one day if I have children they’ll wonder why their mother has scars, you’re not alone, but children are much more intuitive and understanding than they’re given credit for, and in all likelihood, they won’t be traumatised if you say that you went through a hard time. It’s also important to remember that you don’t have to explain your scars if you don’t want to, your past is yours and you don’t owe anyone an explanation.
If you’re struggling with self-harm I have an article on self-harm and suicidal ideations, additionally, there are some websites below which might be helpful. Please stay safe.
https://www.mind.org.uk/information-support/types-of-mental-health-problems/self-harm/useful-contacts/#.Wz9bodJKhPY
https://www.selfinjurysupport.org.uk/help-and-support-with-self-injury/cass-womens-self-injury-helpline-0808-800-8088/
Self-harm scars can be difficult enough to explain to adults, but if there’s a child in your life asking about them it can be overwhelming trying to figure out how to talk to them. There are several options for dealing with this predicament, which I will outline below:
1. Make something up- this is often a go-to for people who really don’t know what to say to someone asking them about self-harm. It’s often an automatic fear response, because telling anyone that you intentionally hurt yourself is difficult but trying to explain the complex reasons behind self-harm, and what it is in the first place, to a child, might seem far too difficult. This option is one which I do not discourage, especially if you’re just not ready to speak about it. You don’t owe anyone an explanation from your scars, even your own children or family members.
2. Explain it- this is a difficult one, but I think it’s worthwhile, particularly if you are being asked about scars by your own children/a sibling/family member you see a lot/are close to. Depending on the age-group, there are different ways of explaining self-harm. For younger children, I would recommend saying something along the lines of ‘just like people get sick in their bodies, you can also get sick in your brain, and that’s what gave me scars’, additionally, if you have recovered I would recommend adding the comforting sentence ‘but I’m doing better now’. Usually younger children won’t ask further questions, and it’s not necessary to get into all the details. Being as calm as possible and speaking in an age-appropriate but frank way will usually ensure that a child feels their questions have been answered. Older children might be ready to hear more about mental illness, and so it might be a good idea to have a longer conversation with them about how emotions and thoughts can lead to problems, including self-harm. What is important to remember is that self-harm is nothing to be ashamed of, and neither is mental illness, speaking openly and honestly to your children about mental health and your own experiences can actually be beneficial in encouraging children and young adults to speak about their own problems, and it makes it more likely that they will go to you in the future if they are struggling.
3. Tell their parents- if the child is not your own then you might consider talking to their parents about your self-harm scars. If you politely mention that their child has asked about the scars, and explain the situation, you can leave the decision of whether or not to explain it to their child to the parents. Some parents may want their children to be informed, whereas others might not think it appropriate to tell their children about self-harm until they are older. For this reason, I feel it is more respectful to ask a parent how they want to handle the situation than to tell the child about it yourself.
Given that we are on the topic of self-harm scars, another important thing to note is that showing self-harm scars is alright. If you chose to wear clothing that shows your scars that’s your decision and you do not need to explain yourself to anyone. On the other hand, showing fresh wounds may be a different matter. One issue with showing wounds is that these can be distressing as they are clearly recent injuries. On the other hand, on a hot day you should not have to overheat because of your self-harm. At the end of the day, what you should be focusing on is recovery and staying safe, not what others might think or worries about how to explain scars. If you have the same worry I do, that one day if I have children they’ll wonder why their mother has scars, you’re not alone, but children are much more intuitive and understanding than they’re given credit for, and in all likelihood, they won’t be traumatised if you say that you went through a hard time. It’s also important to remember that you don’t have to explain your scars if you don’t want to, your past is yours and you don’t owe anyone an explanation.
If you’re struggling with self-harm I have an article on self-harm and suicidal ideations, additionally, there are some websites below which might be helpful. Please stay safe.
https://www.mind.org.uk/information-support/types-of-mental-health-problems/self-harm/useful-contacts/#.Wz9bodJKhPY
https://www.selfinjurysupport.org.uk/help-and-support-with-self-injury/cass-womens-self-injury-helpline-0808-800-8088/
Short-term coping with emotional/mental health problems
So, most of us know that severe emotional/mental health problems are long-term conditions that often require professional intervention, and I would always recommend that someone who is struggling speak to their GP or call an emergency hotline (see the bottom of this article). Sometimes, however, waiting lists are long and quick relief is needed. In these times it is very tempting to use unhealthy coping mechanisms, from isolating oneself to even hurting yourself. While these methods are tempting and often cause short term relief, they will almost always in the long term cause more problems and make the situation worse. Imagine trying to cover an annoying sound with another louder sound. Sure, you won’t be able to hear the annoying sound, but you’ll have another sound pounding on your eardrums. So, healthy coping mechanisms are a much better option. What healthy mechanisms are there? Well, actually a lot. What will work for one person may not work for another, so it often takes a bit of trial and error to find the methods that work best for you, but I’ll outline a few that I’ve heard of and/or found helpful.
1. Music- music has definitely been a lifeline for me, and although it might sound cliché, I genuinely feel understood by certain artists, and some songs can just make me feel less alone when I’m feeling stressed or anxious. I would recommend making a playlist that you can listen to when you’re feeling bad. For some people, it’s helpful to have upbeat happy songs, but for others, including myself, sadder songs might actually be helpful as they can make you feel less alone and allow you to address your feelings in a healthy way. My playlist is just called Mental Health, but I’m sure many people can be way more imaginative than that and come up with better names. Some of the songs I have which deal with anxiety, depression, suicide and eating disorders include: Migraine, Twenty-One Pilots; Courage, Superchick; Car Radio, Twenty-One Pilots; Anti-D, The Wombats, Everything’s Not Lost, Coldplay. These songs are helpful for feeling understood and even taking a minute to think about your feelings if you feel able to face them head on. More upbeat songs are, I probably don’t need to tell you, much better for distraction, so you might want to go with songs that make you feel confident or happy, like pop songs you listened to as a child, or a party playlist. A word of warning about going down the sad song route is that it can sometimes make you feel worse as it can make you think about negative things.
2. Creative pursuits- writing, drawing and making things are all brilliant ways to express yourself and/or distract yourself. Sometimes, especially if you’re feeling depressed, it can be difficult to summon the motivation needed to be creative, but if you’re able to do this I promise you it will be worthwhile. Seeing something you’ve been able to make can greatly improve confidence, and it is almost guaranteed to take your mind of things at least for a little while. It can also provide an opening for talking to someone about what you’re going through if you find it difficult to say it out loud.
3. Inform yourself- learning about what might be going on in your head can be very useful. Sometimes one of the worst things about going through an emotional/mental health problem is not being able to understand what’s happening. Looking online can also show you that you’re not alone, it is very likely that many other people will have been through the same thing that you are going through, and if you want to there are many chatrooms and Facebook groups where you can get support. Being informed can also help your GP if you decide to try and get professional help; having filled in online mental health tests and/or found websites describing what you’re going through can help you and your GP understand what you’re going through and what help you might need. Of course, not all online tests/websites will be totally accurate, and self-diagnosis is not something I would recommend, so never use a test to tell you what’s wrong, use it as a possible indicator of the sort of problems you’re dealing with, which you can go through with professionals to come up with a diagnosis and/or treatment plan.
4. STAY SAFE! - if there’s one thing I want you to take from this article it’s to stay safe. Although it can be unbelievably tempting to do harmful things to make yourself feel better, it is never the right solution. That’s important, so I’ll say it again. It is never the right solution. No matter how bad you might think things are, no matter how much you might want to punish yourself or get short term relief, I can promise you that, in the long term, staying strong and being safe is the only way to actually recover from emotional/mental health problems. The reason for this is that unhealthy coping mechanisms often give a short term hit of endorphins/dopamine, and very short-term relief, which you’ll end up getting used to and maybe dependent on. This adds an extra problem to your life; you’re now dealing with self-harm, alcohol/drug dependence, physical problems, etc. I know of no-one who has been able to lead a happy life using unhealthy coping mechanisms. If you are already dealing with any kind of addiction/self-harm/eating disorder don’t lose hope, there is a lot of help out there and you definitely can get better. One way to stay safe is to talk to someone if you feel like doing something dangerous, this can help you to express your emotions in a healthy way and can take some of the burden off yourself. Knowing that people are there for you can also be very helpful. Another way to be safe is to indulge in self-care. Want to self-harm? Massage the areas you want to hurt, surround yourself with different senses, such as cold water and nice smells. This allows your body some relief through different sensations and can help alleviate tension. Another useful way of staying safe is to set yourself rules. For example, I have a rule that if I want to throw up I have to wait twenty minutes. Most of the time the urge fades in that time. Another rule could be having to do two distracting activities before doing anything unhealthy. This isn’t an extensive list, so I encourage you to do some internet searching to find other healthy coping mechanisms. Young-mind’s BEAT and other mental health websites can be useful.
Here are some helplines which may be helpful:
Papyrus – (for people under 35) 0800 068 41 41
Childline – (for children and young people under 19) 0800 1111
Anxiety UK- 03444 775 774
OCD Action- 0845 390 6232
SANEline: 0300 304 7000 (daily, 4.30-10.30pm)
Helpful websites:
For Depression- www.depressionalliance.org
For Panic/Anxiety- www.nopanic.org.uk
So, most of us know that severe emotional/mental health problems are long-term conditions that often require professional intervention, and I would always recommend that someone who is struggling speak to their GP or call an emergency hotline (see the bottom of this article). Sometimes, however, waiting lists are long and quick relief is needed. In these times it is very tempting to use unhealthy coping mechanisms, from isolating oneself to even hurting yourself. While these methods are tempting and often cause short term relief, they will almost always in the long term cause more problems and make the situation worse. Imagine trying to cover an annoying sound with another louder sound. Sure, you won’t be able to hear the annoying sound, but you’ll have another sound pounding on your eardrums. So, healthy coping mechanisms are a much better option. What healthy mechanisms are there? Well, actually a lot. What will work for one person may not work for another, so it often takes a bit of trial and error to find the methods that work best for you, but I’ll outline a few that I’ve heard of and/or found helpful.
1. Music- music has definitely been a lifeline for me, and although it might sound cliché, I genuinely feel understood by certain artists, and some songs can just make me feel less alone when I’m feeling stressed or anxious. I would recommend making a playlist that you can listen to when you’re feeling bad. For some people, it’s helpful to have upbeat happy songs, but for others, including myself, sadder songs might actually be helpful as they can make you feel less alone and allow you to address your feelings in a healthy way. My playlist is just called Mental Health, but I’m sure many people can be way more imaginative than that and come up with better names. Some of the songs I have which deal with anxiety, depression, suicide and eating disorders include: Migraine, Twenty-One Pilots; Courage, Superchick; Car Radio, Twenty-One Pilots; Anti-D, The Wombats, Everything’s Not Lost, Coldplay. These songs are helpful for feeling understood and even taking a minute to think about your feelings if you feel able to face them head on. More upbeat songs are, I probably don’t need to tell you, much better for distraction, so you might want to go with songs that make you feel confident or happy, like pop songs you listened to as a child, or a party playlist. A word of warning about going down the sad song route is that it can sometimes make you feel worse as it can make you think about negative things.
2. Creative pursuits- writing, drawing and making things are all brilliant ways to express yourself and/or distract yourself. Sometimes, especially if you’re feeling depressed, it can be difficult to summon the motivation needed to be creative, but if you’re able to do this I promise you it will be worthwhile. Seeing something you’ve been able to make can greatly improve confidence, and it is almost guaranteed to take your mind of things at least for a little while. It can also provide an opening for talking to someone about what you’re going through if you find it difficult to say it out loud.
3. Inform yourself- learning about what might be going on in your head can be very useful. Sometimes one of the worst things about going through an emotional/mental health problem is not being able to understand what’s happening. Looking online can also show you that you’re not alone, it is very likely that many other people will have been through the same thing that you are going through, and if you want to there are many chatrooms and Facebook groups where you can get support. Being informed can also help your GP if you decide to try and get professional help; having filled in online mental health tests and/or found websites describing what you’re going through can help you and your GP understand what you’re going through and what help you might need. Of course, not all online tests/websites will be totally accurate, and self-diagnosis is not something I would recommend, so never use a test to tell you what’s wrong, use it as a possible indicator of the sort of problems you’re dealing with, which you can go through with professionals to come up with a diagnosis and/or treatment plan.
4. STAY SAFE! - if there’s one thing I want you to take from this article it’s to stay safe. Although it can be unbelievably tempting to do harmful things to make yourself feel better, it is never the right solution. That’s important, so I’ll say it again. It is never the right solution. No matter how bad you might think things are, no matter how much you might want to punish yourself or get short term relief, I can promise you that, in the long term, staying strong and being safe is the only way to actually recover from emotional/mental health problems. The reason for this is that unhealthy coping mechanisms often give a short term hit of endorphins/dopamine, and very short-term relief, which you’ll end up getting used to and maybe dependent on. This adds an extra problem to your life; you’re now dealing with self-harm, alcohol/drug dependence, physical problems, etc. I know of no-one who has been able to lead a happy life using unhealthy coping mechanisms. If you are already dealing with any kind of addiction/self-harm/eating disorder don’t lose hope, there is a lot of help out there and you definitely can get better. One way to stay safe is to talk to someone if you feel like doing something dangerous, this can help you to express your emotions in a healthy way and can take some of the burden off yourself. Knowing that people are there for you can also be very helpful. Another way to be safe is to indulge in self-care. Want to self-harm? Massage the areas you want to hurt, surround yourself with different senses, such as cold water and nice smells. This allows your body some relief through different sensations and can help alleviate tension. Another useful way of staying safe is to set yourself rules. For example, I have a rule that if I want to throw up I have to wait twenty minutes. Most of the time the urge fades in that time. Another rule could be having to do two distracting activities before doing anything unhealthy. This isn’t an extensive list, so I encourage you to do some internet searching to find other healthy coping mechanisms. Young-mind’s BEAT and other mental health websites can be useful.
Here are some helplines which may be helpful:
Papyrus – (for people under 35) 0800 068 41 41
Childline – (for children and young people under 19) 0800 1111
Anxiety UK- 03444 775 774
OCD Action- 0845 390 6232
SANEline: 0300 304 7000 (daily, 4.30-10.30pm)
Helpful websites:
For Depression- www.depressionalliance.org
For Panic/Anxiety- www.nopanic.org.uk
Intrusive thoughts
Radio static can sometimes interrupt the normal chattering on the radio. Sometimes its faint and barely noticeable, other times its so loud you can no longer hear the program you tuned in for. This radio chatter is just meaningless noise, but that doesn’t mean its easy to ignore. This is what it can be like to have intrusive thoughts; it’s like you’re trying to listen to the radio, but all you can hear is horrifically loud static. Sometimes its difficult to know what noises are part of the program, and which are just static.
So, what are intrusive thoughts? These are unwanted mental images, thoughts or urges that are involuntary and can come into one’s mind due to a trigger, or even for no reason at all. They are sometimes also referred to as obsessions when they are reoccurring and take up a significant amount of a person’s time, as well as when they cause distress. Common obsessions can be broken down into four main types:
The above obsessions are linked to the condition obsessive compulsive disorder (OCD), which often comes along with compulsions, such as having to clean ones hands (due to contamination obsessions), praying/mental compulsions such as repeating a calming phrase in one’s head (due to harm/sexual/religious obsessions), spending hours a day checking that things are right/rearranging/reorganising things (due to symmetry/completeness obsessions).
Intrusive thoughts are not only common to OCD but are actually common for most healthy people from time to time. The difference between ‘normal’ intrusive thoughts and OCD/mental disordered intrusive thoughts, is that in the latter case individuals may pay too much attention to these thoughts, thinking that they are meaningful and might suggest something about their character. For example, after watching a disturbing documentary on sexual abuse someone might have the recurring intrusive image of rape/other similar unwanted thoughts. Someone without ‘problems with intrusive thoughts’ will be able to quickly dismiss this as just a consequences of having watched something that bothered them. Someone with a mental health problem like OCD, however, may find these images particularly distressing and be unable to control the anxiety they cause, and they may think that having these thoughts/images in their minds makes them a pervert or means that they might want to do the things they have seen in the documentary. This can sometimes spiral into full blown sexual obsessions, whereby people have intense fears of being a sexual deviant/evil.
Another possible case of intrusive thoughts might begin with being struck down by a terrible illness that made you feel terrible. After this it is possible that a person may have intrusive thoughts such as ‘I am ill’, ‘I have cancer’, and may even have intrusive images of being ill which cause them a lot of distress. This might lead them to have to decontaminate every part of their house and might take hours out of their day. This would be considered OCD. But OCD doesn’t just involve overt compulsions; mental compulsions are also present in a type of OCD called ‘pure OCD’. In this case, people have mental rituals and compulsions that they perform to calm themselves down/get rid of compulsions/prevent some awful thing from happening. For example, someone might be afraid that they will die in a plane crash and so may have to repeat a certain prayer in their head to alleviate large amounts of anxiety.
A big theme that emerges throughout intrusive thoughts is that they are intrusive; they are not voluntary, and people are generally very distressed by them. This is something that I want to remind people who are suffering with intrusive thoughts of, because its very easy to think of yourself as a bad person for having ‘bad’ thoughts, but the truth is, thoughts are just thoughts, and they don’t necessarily represent what you want or the truth about the world; it’s just radio static.
Here are some useful links about intrusive thoughts and OCD:
https://www.nhs.uk/conditions/obsessive-compulsive-disorder-ocd/#symptoms-of-ocd
https://moodsmith.com/intrusive-thoughts/
https://www.psychologytoday.com/gb/blog/am-i-normal/201110/intrusive-thoughts-normal-or-not
Radio static can sometimes interrupt the normal chattering on the radio. Sometimes its faint and barely noticeable, other times its so loud you can no longer hear the program you tuned in for. This radio chatter is just meaningless noise, but that doesn’t mean its easy to ignore. This is what it can be like to have intrusive thoughts; it’s like you’re trying to listen to the radio, but all you can hear is horrifically loud static. Sometimes its difficult to know what noises are part of the program, and which are just static.
So, what are intrusive thoughts? These are unwanted mental images, thoughts or urges that are involuntary and can come into one’s mind due to a trigger, or even for no reason at all. They are sometimes also referred to as obsessions when they are reoccurring and take up a significant amount of a person’s time, as well as when they cause distress. Common obsessions can be broken down into four main types:
- Contamination obsessions, e.g. the fear of germs and getting an illness.
- Harm obsessions, e.g. the fear that you will cause harm to someone else or yourself, often accompanied by intrusive images of violence and even urges to do things that are completely out of character, like push someone in front of a train or stab oneself.
- Sexual and religious obsessions, e.g. frequent unwanted images of sexual content, fears of being a paedophile even when you are not, intrusive blasphemous thoughts, fears of going to hell and other disturbing/morally out of character content.
- Symmetry/completeness obsessions, e.g. the intense urge to have things perfectly symmetrical, the inability to leave things unfinished, an intensely uncomfortable feeling of anxiety when things are not ‘just so’.
The above obsessions are linked to the condition obsessive compulsive disorder (OCD), which often comes along with compulsions, such as having to clean ones hands (due to contamination obsessions), praying/mental compulsions such as repeating a calming phrase in one’s head (due to harm/sexual/religious obsessions), spending hours a day checking that things are right/rearranging/reorganising things (due to symmetry/completeness obsessions).
Intrusive thoughts are not only common to OCD but are actually common for most healthy people from time to time. The difference between ‘normal’ intrusive thoughts and OCD/mental disordered intrusive thoughts, is that in the latter case individuals may pay too much attention to these thoughts, thinking that they are meaningful and might suggest something about their character. For example, after watching a disturbing documentary on sexual abuse someone might have the recurring intrusive image of rape/other similar unwanted thoughts. Someone without ‘problems with intrusive thoughts’ will be able to quickly dismiss this as just a consequences of having watched something that bothered them. Someone with a mental health problem like OCD, however, may find these images particularly distressing and be unable to control the anxiety they cause, and they may think that having these thoughts/images in their minds makes them a pervert or means that they might want to do the things they have seen in the documentary. This can sometimes spiral into full blown sexual obsessions, whereby people have intense fears of being a sexual deviant/evil.
Another possible case of intrusive thoughts might begin with being struck down by a terrible illness that made you feel terrible. After this it is possible that a person may have intrusive thoughts such as ‘I am ill’, ‘I have cancer’, and may even have intrusive images of being ill which cause them a lot of distress. This might lead them to have to decontaminate every part of their house and might take hours out of their day. This would be considered OCD. But OCD doesn’t just involve overt compulsions; mental compulsions are also present in a type of OCD called ‘pure OCD’. In this case, people have mental rituals and compulsions that they perform to calm themselves down/get rid of compulsions/prevent some awful thing from happening. For example, someone might be afraid that they will die in a plane crash and so may have to repeat a certain prayer in their head to alleviate large amounts of anxiety.
A big theme that emerges throughout intrusive thoughts is that they are intrusive; they are not voluntary, and people are generally very distressed by them. This is something that I want to remind people who are suffering with intrusive thoughts of, because its very easy to think of yourself as a bad person for having ‘bad’ thoughts, but the truth is, thoughts are just thoughts, and they don’t necessarily represent what you want or the truth about the world; it’s just radio static.
Here are some useful links about intrusive thoughts and OCD:
https://www.nhs.uk/conditions/obsessive-compulsive-disorder-ocd/#symptoms-of-ocd
https://moodsmith.com/intrusive-thoughts/
https://www.psychologytoday.com/gb/blog/am-i-normal/201110/intrusive-thoughts-normal-or-not
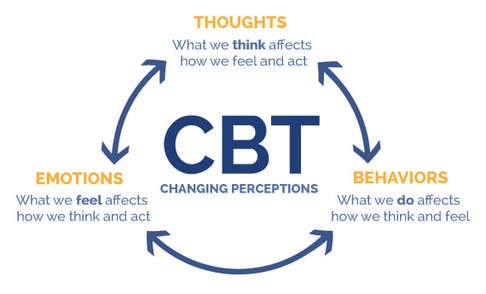
CBT: How it works and why it's good
Cognitive Behavioral Therapy (CBT) is a common treatment for a variety of common mental health disorders, from depression to anxiety and eating disorders. This approach combines cognitive components with, you guessed it, behavioral components. The cognitive component of CBT involves a variety of methods for tackling maladaptive/dysfunctional thought patterns and schema's underlying a multitude of problems. Schema's refer to mental templates/expectations people have for certain situations. For example, one unhelpful schema might involve an expectation that you will fail in social situations. This leads to certain beliefs, such as "I am awkward around people" and negative automatic thoughts (NAT's) such as "She thinks I'm annoying". CBT first aims to tackle the most easily accessible and conscious of these mental processes; NAT's. One way of doing this is through a thought table, where you would write down a situation, the thoughts and emotions associated with this situation and what behaviors this led to. For example, someone with anorexia binge/purge sub-type might write 'Situation: eating chocolate (subjective binge). Thoughts: I shouldn't have eaten that. That was greedy. It'll make me fat. Emotions: guilt, sadness, anxiety. Behaviors: purging, exercise'. Once common patterns of thoughts, behaviors and emotions are established, it's time to look at the evidence and challenge your automatic negative thoughts. One way of doing this is to write alternative, more helpful thoughts that you could associate with the situation. For example, in the previous case a more helpful thought would be 'It's normal to eat chocolate. Most people have treats sometimes'. With regards to the last thought an experiment whereby the person tracks their weight before and after eating something 'bad' might be a useful way of demonstrating that the thought is inaccurate. This method of tackling eating disorders is recommended for after a person is already in recovery, as it requires a lot of hard work and might not always be possible for someone who is very ill.
CBT is very useful for anxiety disorders and depression, being one of the leading treatments for these disorders. With regards to anxiety, it teaches a person to challenge their anxiety provoking thoughts and engage in experiments to show themselves that the bad things they are worried about will not happen/they can endure them. For example, an anxiety provoking thought might be 'I'm going to embarrass myself if I go out', which may lead to avoidance of many social situations. CBT would encourage someone to expose themselves to this situation by going out, at first maybe just to see one or two people, so that they can see that their fears will not be realized. The thinking behind this relates to Mowrer's Two-Factor theory of anxiety. This involves classical conditioning, where something which doesn't provoke anxiety is paired with a naturally anxiety provoking stimulus (such as pain or unpleasant sensations) and so ends up causing anxiety in itself. This is perpetuated by operant conditioning, where avoidance behaviors are negatively reinforced (a negative stimulus is removed) because they reduce anxiety. By getting people to expose themselves to anxiety provoking situations, it is hoped that the conditioned response (fear in response to a previously neutral stimulus) will be extinguished. This is a bit complicated, so here's an example to help clarify what it means. Someone might experience the unpleasant sensation of embarrassment (the unconditioned stimulus) due to a social faux-par (a neutral stimulus, e.g. messing up their lines when speaking in front of a crowd) which will lead to a conditioned response (fear of talking in front of people), meaning that the previously neutral stimulus is now a conditioned stimulus that can make someone anxious in itself. This could lead to avoidance of social situations, which will reduce anxiety and so negatively reinforce avoidance. If you are suffering from anxiety, it might sound pretty insane for me to ask you to expose yourself to a feared situation/stimulus. I'm not going to ask you to jump right into the deep end and do that, but one thing which can be useful and is a common part of CBT is to gradually expose yourself to the things that cause anxiety. For example, you might start by visualizing a feared situation in as much detail as you can. You might then write about this situation/role play it with a friend/family member. When you feel ready you might want to enter the feared situation with a trusted chaperone, and then eventually you may feel ready to tackle the situation by yourself. This method has proven very helpful for many people suffering from anxiety. In studies comparing drug treatment to CBT for anxiety, CBT generally comes out on top. This isn't to say that medication might not be useful, particularly if your symptoms are severe. It may be that a combination of CBT and medication would be helpful.
With depression, CBT can be very useful for tackling negative thinking patterns. For example, it teaches people to recognize and challenge a variety of common cognitive distortions present in depression. These include personalisation (thinking that bad things are your fault), catastrophic thinking ("everything is awful"), filtering (focusing only on the negative things and ignoring the positive). One way of doing this is to write on a thought table all of the thoughts that you have been experiencing and see whether they fit into any of the cognitive distortions. For example, a negative thought might be "I can't do anything right", which would be an example of filtering. In order to challenge this distortion, it is helpful to write an alternative thought as well as evidence for an against the negative thought. For example, "I can't do anything right" can be challenged by writing down all of your achievements, even if they are only small. Getting out bed is a genuine achievement when you're suffering from severe depression, take note of the little things. People who receive CBT for depression often recover very well and are less likely to relapse. So, if you are suffering from some mild symptoms of depression, doing some self-help CBT could be very beneficial. If you're suffering from a more severe mental health disorder, such as full blown depression/anxiety, that is impacting negatively on your everyday life and ability to function, I would recommend that you get professional help.
A major benefit of CBT is that it allows you to recognize and tackle the underlying negative thought patterns that might be contributing to your mental health problems. While medication is sometimes necessary and often very helpful, in some cases it can be considered to be just masking the underlying problems rather than tackling them, which is why CBT is often combined with pharmacological methods to treat mental health problems. Even if you do not suffer from mental health problems, CBT can be an excellent way to look after and monitor your general mental health and improve your emotional well-being. Physical health is often emphasized as being very important, and it is, but so is mental health. Everyone has mental health, whether or not they have a mental health disorder, and it is important that we all take care of it.
Here are some helpful links for doing CBT exercises and getting professional help:
https://www.mind.org.uk/information-support/drugs-and-treatments/cognitive-behavioural-therapy-cbt/#.WuGng4jwZPY
https://www.nhs.uk/conditions/cognitive-behavioural-therapy-cbt/
https://www.simplypsychology.org/cognitive-therapy.html
https://positivepsychologyprogram.com/cbt-cognitive-behavioral-therapy-techniques-worksheets/
Here is a worksheet for tackling dysfunction thoughts:
Cognitive Behavioral Therapy (CBT) is a common treatment for a variety of common mental health disorders, from depression to anxiety and eating disorders. This approach combines cognitive components with, you guessed it, behavioral components. The cognitive component of CBT involves a variety of methods for tackling maladaptive/dysfunctional thought patterns and schema's underlying a multitude of problems. Schema's refer to mental templates/expectations people have for certain situations. For example, one unhelpful schema might involve an expectation that you will fail in social situations. This leads to certain beliefs, such as "I am awkward around people" and negative automatic thoughts (NAT's) such as "She thinks I'm annoying". CBT first aims to tackle the most easily accessible and conscious of these mental processes; NAT's. One way of doing this is through a thought table, where you would write down a situation, the thoughts and emotions associated with this situation and what behaviors this led to. For example, someone with anorexia binge/purge sub-type might write 'Situation: eating chocolate (subjective binge). Thoughts: I shouldn't have eaten that. That was greedy. It'll make me fat. Emotions: guilt, sadness, anxiety. Behaviors: purging, exercise'. Once common patterns of thoughts, behaviors and emotions are established, it's time to look at the evidence and challenge your automatic negative thoughts. One way of doing this is to write alternative, more helpful thoughts that you could associate with the situation. For example, in the previous case a more helpful thought would be 'It's normal to eat chocolate. Most people have treats sometimes'. With regards to the last thought an experiment whereby the person tracks their weight before and after eating something 'bad' might be a useful way of demonstrating that the thought is inaccurate. This method of tackling eating disorders is recommended for after a person is already in recovery, as it requires a lot of hard work and might not always be possible for someone who is very ill.
CBT is very useful for anxiety disorders and depression, being one of the leading treatments for these disorders. With regards to anxiety, it teaches a person to challenge their anxiety provoking thoughts and engage in experiments to show themselves that the bad things they are worried about will not happen/they can endure them. For example, an anxiety provoking thought might be 'I'm going to embarrass myself if I go out', which may lead to avoidance of many social situations. CBT would encourage someone to expose themselves to this situation by going out, at first maybe just to see one or two people, so that they can see that their fears will not be realized. The thinking behind this relates to Mowrer's Two-Factor theory of anxiety. This involves classical conditioning, where something which doesn't provoke anxiety is paired with a naturally anxiety provoking stimulus (such as pain or unpleasant sensations) and so ends up causing anxiety in itself. This is perpetuated by operant conditioning, where avoidance behaviors are negatively reinforced (a negative stimulus is removed) because they reduce anxiety. By getting people to expose themselves to anxiety provoking situations, it is hoped that the conditioned response (fear in response to a previously neutral stimulus) will be extinguished. This is a bit complicated, so here's an example to help clarify what it means. Someone might experience the unpleasant sensation of embarrassment (the unconditioned stimulus) due to a social faux-par (a neutral stimulus, e.g. messing up their lines when speaking in front of a crowd) which will lead to a conditioned response (fear of talking in front of people), meaning that the previously neutral stimulus is now a conditioned stimulus that can make someone anxious in itself. This could lead to avoidance of social situations, which will reduce anxiety and so negatively reinforce avoidance. If you are suffering from anxiety, it might sound pretty insane for me to ask you to expose yourself to a feared situation/stimulus. I'm not going to ask you to jump right into the deep end and do that, but one thing which can be useful and is a common part of CBT is to gradually expose yourself to the things that cause anxiety. For example, you might start by visualizing a feared situation in as much detail as you can. You might then write about this situation/role play it with a friend/family member. When you feel ready you might want to enter the feared situation with a trusted chaperone, and then eventually you may feel ready to tackle the situation by yourself. This method has proven very helpful for many people suffering from anxiety. In studies comparing drug treatment to CBT for anxiety, CBT generally comes out on top. This isn't to say that medication might not be useful, particularly if your symptoms are severe. It may be that a combination of CBT and medication would be helpful.
With depression, CBT can be very useful for tackling negative thinking patterns. For example, it teaches people to recognize and challenge a variety of common cognitive distortions present in depression. These include personalisation (thinking that bad things are your fault), catastrophic thinking ("everything is awful"), filtering (focusing only on the negative things and ignoring the positive). One way of doing this is to write on a thought table all of the thoughts that you have been experiencing and see whether they fit into any of the cognitive distortions. For example, a negative thought might be "I can't do anything right", which would be an example of filtering. In order to challenge this distortion, it is helpful to write an alternative thought as well as evidence for an against the negative thought. For example, "I can't do anything right" can be challenged by writing down all of your achievements, even if they are only small. Getting out bed is a genuine achievement when you're suffering from severe depression, take note of the little things. People who receive CBT for depression often recover very well and are less likely to relapse. So, if you are suffering from some mild symptoms of depression, doing some self-help CBT could be very beneficial. If you're suffering from a more severe mental health disorder, such as full blown depression/anxiety, that is impacting negatively on your everyday life and ability to function, I would recommend that you get professional help.
A major benefit of CBT is that it allows you to recognize and tackle the underlying negative thought patterns that might be contributing to your mental health problems. While medication is sometimes necessary and often very helpful, in some cases it can be considered to be just masking the underlying problems rather than tackling them, which is why CBT is often combined with pharmacological methods to treat mental health problems. Even if you do not suffer from mental health problems, CBT can be an excellent way to look after and monitor your general mental health and improve your emotional well-being. Physical health is often emphasized as being very important, and it is, but so is mental health. Everyone has mental health, whether or not they have a mental health disorder, and it is important that we all take care of it.
Here are some helpful links for doing CBT exercises and getting professional help:
https://www.mind.org.uk/information-support/drugs-and-treatments/cognitive-behavioural-therapy-cbt/#.WuGng4jwZPY
https://www.nhs.uk/conditions/cognitive-behavioural-therapy-cbt/
https://www.simplypsychology.org/cognitive-therapy.html
https://positivepsychologyprogram.com/cbt-cognitive-behavioral-therapy-techniques-worksheets/
Here is a worksheet for tackling dysfunction thoughts:
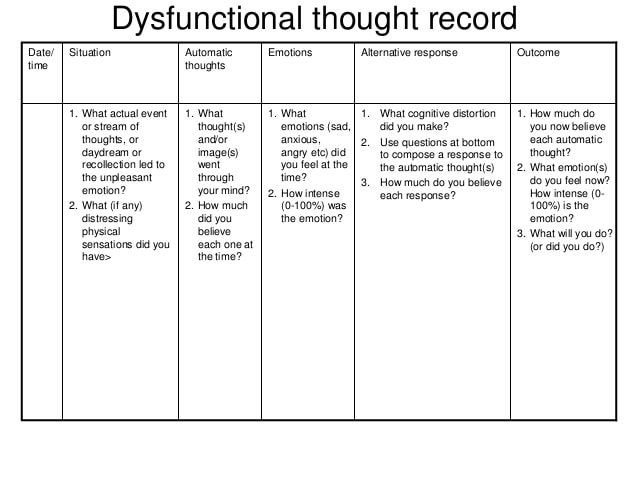

Pro-Ana/pro-mia sites and their dangers
Pro-ana and pro-mia sites are online sites that promote anorexia and bulimia, often referring to these conditions as lifestyle choices. On these sites are 'tips', such as diet plans and even tips on how to purge. Content of these websites includes thinspiration (photos and quotes), calculations such as BMI and calories burnt and 'tips and tricks' (Norris et al., 2006). Many studies have shown that after viewing such websites even healthy participants report lower self-esteem and lower mood, so imagine how triggering and damaging such material can be for someone at risk of an eating disorder, or for someone trying to recover. Currently there are some regulations of these sites, and they have been banned in France. The problem is, the internet is very hard to regulate, and many sites will use covert methods to not be detected, such as stating that you should not starve yourself/they do not promote eating disorders. When I was ill I mostly used Tumblr for thinspiration and ideas on how to lose weight. This included pictures of emancipated girls and messages such as "skip dinner, wake up thinner". I never went on official pro-ana/pro-mia sites, so I decided to investigate and see what they were really like.
One site I found has, in big red letters, the statement "HEAVY DIETARY CHANGES AND EXERCISE CAN BE A DEADLY HAZARD TO YOUR LIFE. NOTHING IS MORE PRECIOUS THAN YOUR LIFE. PLEASE MAKE SUSTAINABLE CHANGES ONLY", which is great. However, also on the website is the 'Mary-Kate Ashley' challenge, where you don't eat for a day (by the way, Mary-Kate Ashley suffered from severe anorexia), and a multitude of other diet plans, including the 'super anorexic diet', where you only eat an apple a day. I'm pretty sure that encouraging people to follow these plans is promoting eating disorders. There is a point system on this website where you get 2 points for purging on a binge. This made me really angry, for several reasons. Firstly, obviously, it's just stupid and unhealthy to promote this kind of eating. Secondly, if you're going to promote anorexia, at least admit what you're doing and don't pretend that it's anything else. Thirdly, this was easy to find, as is a lot of thinspiration. Anyone could just type in pro-ana and get it, including vulnerable young people at risk of eating disorders, the very people most likely to look for this stuff.
The thing is, while it's obviously harmful to run sites like this, recommended prison sentences for the people who run such sites don't seem like the right move. As the charity BEAT states, this would just be criminalizing people who are ill (Saul, 2015). So, what should be done about these sites? Well, one thing tumblr does that is good is that if you type in 'thinspo', you will get a page asking you if everything's okay and signposting you to call NEDA (an eating disorder helpline), of course, this doesn't mean you can't still view the results, but it does highlight to a person that they might be doing something dangerous, and points out where they might be able to get help. Something which I feel is the most feasible way of actually helping people is to educate them about the dangers of eating disorders and pro-ana/pro-mia material. Regulation is very difficult, and it's likely that, no matter how much government authorities try, there will always be some dark depths of the internet where one can go to get their fill of thinspiration. With that in mind, here's just a few major dangers of eating disorders (for more of an in-depth look at these, see the article below):
Without iron in your diet you are at risk of anemia (lack of healthy red blood cells), which can make you tired, give you irregular heartbeats, headaches and dizziness. Most of the recommended diets on the first site I found certainly wouldn't provide any iron, or any protein, or any vitamins, or really, well...anything, for that matter. Fat is often seen as a dirty word, but it's vitally important for our bodies and brains, it helps us absorb nutrients, encourages cell growth and keeps us warm. Omega-3 fatty acid is also especially implicated in brain function, so it's important to try and get a healthy amount of this in your diet, which you cannot get if you are restricting. Calcium is also very important for your body; it helps regulate muscle contractions, contributes to healthy teeth and bones and makes sure the blood clots normally. Lack of calcium could lead to Osteoporosis (fragile bones). Foods which have calcium in them include dairy products (milk, cheese, etc.), green leafy vegetables like spinach (which also has iron in it, so two birds...), soya beans, tofu, a lot of soya products (I recommend chocolate soya milk, it's good), nuts and anything made with fortified flour. There's a lot of good sources of calcium in food, and in order to maintain healthy amounts you need to get enough calcium from different sources. Other important vitamins include Vitamin K (which helps keep skin and eyes healthy and strengthens the immune system) and Vitamin C (which helps with wound healing, maintaining healthy skin and bones and protecting cells). Not eating enough means your body won't get the vital vitamins and minerals it needs to function properly, this is obviously horrible for your physical health, but it's also detrimental to your mental health.
When your body is in starvation mode, it may go into a panic-like state, increasing feelings of anxiety. Depression is also more likely to occur/get worse if your body is malnourished. Many pro-ana/pro-mia sites, and western society in general, might state that being skinny leads to happiness, but the evidence actually suggests that being malnourished is more likely to cause anxiety and depression. The thing is, no matter how much weight you lose, if you're in an ill state of mind such as when suffering from an eating disorder, it will never be enough. You will just want to keep pushing the goalposts and it will never make you feel fulfilled. I have only ever felt fulfilled after regaining weight and focusing on other areas of my life, and this is the case for anyone recovering from an eating disorder. I may be wrong, but I know of no case where an eating disorder has led to a happy life, and especially not a happier one than recovery can lead to.
Useful sites:
https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-c/
https://www.independent.co.uk/life-style/health-and-families/health-news/people-running-thinspiration-or-pro-anorexia-websites-in-france-will-now-face-a-prison-sentence-and-10153909.html
https://www.beateatingdisorders.org.uk/
Pro-ana and pro-mia sites are online sites that promote anorexia and bulimia, often referring to these conditions as lifestyle choices. On these sites are 'tips', such as diet plans and even tips on how to purge. Content of these websites includes thinspiration (photos and quotes), calculations such as BMI and calories burnt and 'tips and tricks' (Norris et al., 2006). Many studies have shown that after viewing such websites even healthy participants report lower self-esteem and lower mood, so imagine how triggering and damaging such material can be for someone at risk of an eating disorder, or for someone trying to recover. Currently there are some regulations of these sites, and they have been banned in France. The problem is, the internet is very hard to regulate, and many sites will use covert methods to not be detected, such as stating that you should not starve yourself/they do not promote eating disorders. When I was ill I mostly used Tumblr for thinspiration and ideas on how to lose weight. This included pictures of emancipated girls and messages such as "skip dinner, wake up thinner". I never went on official pro-ana/pro-mia sites, so I decided to investigate and see what they were really like.
One site I found has, in big red letters, the statement "HEAVY DIETARY CHANGES AND EXERCISE CAN BE A DEADLY HAZARD TO YOUR LIFE. NOTHING IS MORE PRECIOUS THAN YOUR LIFE. PLEASE MAKE SUSTAINABLE CHANGES ONLY", which is great. However, also on the website is the 'Mary-Kate Ashley' challenge, where you don't eat for a day (by the way, Mary-Kate Ashley suffered from severe anorexia), and a multitude of other diet plans, including the 'super anorexic diet', where you only eat an apple a day. I'm pretty sure that encouraging people to follow these plans is promoting eating disorders. There is a point system on this website where you get 2 points for purging on a binge. This made me really angry, for several reasons. Firstly, obviously, it's just stupid and unhealthy to promote this kind of eating. Secondly, if you're going to promote anorexia, at least admit what you're doing and don't pretend that it's anything else. Thirdly, this was easy to find, as is a lot of thinspiration. Anyone could just type in pro-ana and get it, including vulnerable young people at risk of eating disorders, the very people most likely to look for this stuff.
The thing is, while it's obviously harmful to run sites like this, recommended prison sentences for the people who run such sites don't seem like the right move. As the charity BEAT states, this would just be criminalizing people who are ill (Saul, 2015). So, what should be done about these sites? Well, one thing tumblr does that is good is that if you type in 'thinspo', you will get a page asking you if everything's okay and signposting you to call NEDA (an eating disorder helpline), of course, this doesn't mean you can't still view the results, but it does highlight to a person that they might be doing something dangerous, and points out where they might be able to get help. Something which I feel is the most feasible way of actually helping people is to educate them about the dangers of eating disorders and pro-ana/pro-mia material. Regulation is very difficult, and it's likely that, no matter how much government authorities try, there will always be some dark depths of the internet where one can go to get their fill of thinspiration. With that in mind, here's just a few major dangers of eating disorders (for more of an in-depth look at these, see the article below):
- Death
- Hair loss
- Low potassium
- Low blood pressure
- Dizziness/fainting
- Loss of concentration
- Anxiety and depression
- Osteoporosis
Without iron in your diet you are at risk of anemia (lack of healthy red blood cells), which can make you tired, give you irregular heartbeats, headaches and dizziness. Most of the recommended diets on the first site I found certainly wouldn't provide any iron, or any protein, or any vitamins, or really, well...anything, for that matter. Fat is often seen as a dirty word, but it's vitally important for our bodies and brains, it helps us absorb nutrients, encourages cell growth and keeps us warm. Omega-3 fatty acid is also especially implicated in brain function, so it's important to try and get a healthy amount of this in your diet, which you cannot get if you are restricting. Calcium is also very important for your body; it helps regulate muscle contractions, contributes to healthy teeth and bones and makes sure the blood clots normally. Lack of calcium could lead to Osteoporosis (fragile bones). Foods which have calcium in them include dairy products (milk, cheese, etc.), green leafy vegetables like spinach (which also has iron in it, so two birds...), soya beans, tofu, a lot of soya products (I recommend chocolate soya milk, it's good), nuts and anything made with fortified flour. There's a lot of good sources of calcium in food, and in order to maintain healthy amounts you need to get enough calcium from different sources. Other important vitamins include Vitamin K (which helps keep skin and eyes healthy and strengthens the immune system) and Vitamin C (which helps with wound healing, maintaining healthy skin and bones and protecting cells). Not eating enough means your body won't get the vital vitamins and minerals it needs to function properly, this is obviously horrible for your physical health, but it's also detrimental to your mental health.
When your body is in starvation mode, it may go into a panic-like state, increasing feelings of anxiety. Depression is also more likely to occur/get worse if your body is malnourished. Many pro-ana/pro-mia sites, and western society in general, might state that being skinny leads to happiness, but the evidence actually suggests that being malnourished is more likely to cause anxiety and depression. The thing is, no matter how much weight you lose, if you're in an ill state of mind such as when suffering from an eating disorder, it will never be enough. You will just want to keep pushing the goalposts and it will never make you feel fulfilled. I have only ever felt fulfilled after regaining weight and focusing on other areas of my life, and this is the case for anyone recovering from an eating disorder. I may be wrong, but I know of no case where an eating disorder has led to a happy life, and especially not a happier one than recovery can lead to.
Useful sites:
https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-c/
https://www.independent.co.uk/life-style/health-and-families/health-news/people-running-thinspiration-or-pro-anorexia-websites-in-france-will-now-face-a-prison-sentence-and-10153909.html
https://www.beateatingdisorders.org.uk/
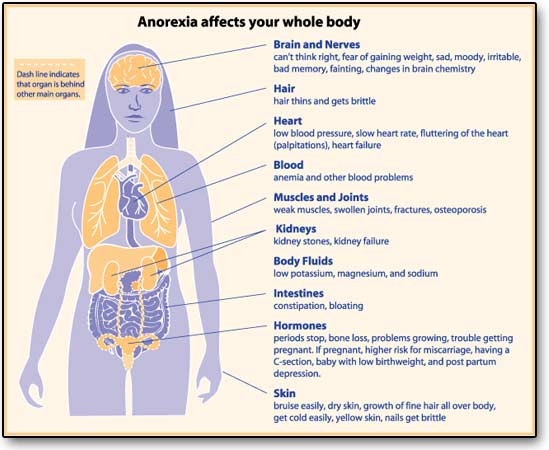
Why eating disorders are so dangerous and why you can recover
Eating disorders, particularly Anorexia, have one of the highest morality rates of any disorder and incur a multitude of awful medical problems, including heart arrhythmia's (irregular heartbeats), kidney problems and osteoporosis. I would say I don't want to scare you, but I do; the risks of EDs are scary. The mortality rate for people with Anorexia is more than 5 times higher than the mortality rate for young females aged 15-34 in the general US population (Keshavia et al., 2014), 3% of people with Anorexia die from medical complications caused by starvation (Signorini et al., 2007), and many other individuals with Anorexia die from suicide (there is an 18 times higher risk of suicide in people with Anorexia according to Kashavia et al., 2014). Malnutrition also causes many other problems, including dry skin, downy hair on the arms, back, face, etc., yellowish tinge to the skin, over-sensitivity to the cold (including purplish extremities due to a lack of oxygen). Low blood pressure often causes individuals to feel dizzy and faint. Vitamin B deficiency is also a big risk and can lead to depression and cognitive changes often seen in people at low weights. One of the biggest and longest standing risks is osteoporosis; if you fail to eat properly during adolescence and early adulthood, when peak bone density should be achieved, you may suffer from weak/fragile bones for the rest of your life, even if you recover. Imbalances in electrolytes, including potassium, can lead to heart arrhythmia's which can be lethal. This is also a big risk in Bulimia, as purging through vomiting and/or laxatives can lead to imbalances in electrolytes. Chronically low potassium levels can lead to kidney damage and renal failure which may require dialysis. Laxative abuse can also cause gastrointestinal problems, damage to the bowels and dehydration. People with Bulimia may also end up with calluses on their hands from using their fingers to throw up, dental problems including cavities and mouth ulcers, and even tears of the throat caused by using objects to throw up. So it is clear how dangerous eating disorders can be, and although Bulimia has a lower mortality rate than Anorexia, people with Bulimia are still twice as likely to die than their non-Bulimic peers (Arceulus et al., 2011).
That's the bad news. The good news is that recovery is very possible! Lowe et al. (2001) found that, 21 years after first seeking treatment, 16% of Anorexic patients were no longer alive, 10% were still suffering, 21% had partially recovered and 51% had fully recovered. This is very promising as it suggests that, even though Anorexia is a very dangerous illness, it is still more likely for people to get better than to not get better. Furthermore, Keel et al. (1999) and Fichter & Quadfleig (2007) found that, at the end of an 11-12 year follow-up, 70% of Bulimic patients were in remission, no longer meeting the criteria for any ED. The earlier an individual is given treatment, the more likely they are to recover. Arcelus (2011) found those who were older when first receiving treatment for Anorexia were more likely to die prematurely. I do not want to pretend that recovery is all rosy; recovery is subjective, and many people who no longer meet diagnostic criteria for an eating disorder still suffer from weight and body-shape concerns, as well as problems with food (Sullivan, 2002). Despite this, it is clear that it is very possible for someone who has suffered from an eating disorder to live a full and happy life. Things may never be the same again, I'm afraid, but they can still be wonderful, and beautiful, and worth fighting for. When I was ill I thought there was no way I could ever be okay, and that I'd end up in a ditch. I wouldn't have believed that a few years later I'd be a healthy weight, relatively happy with myself and enjoying my life. So, to anyone suffering from an ED, if I was able to do it, you definately can. It will not be easy, I won't lie, but it will be worth it. Living with an eating disorder is no way to live.
References and useful links:
Hooley et al. (2016) Abnormal Psychology
https://www.beateatingdisorders.org.uk/
NHS website: eating disorder section
NHS website: BMI calculator
Eating disorders, particularly Anorexia, have one of the highest morality rates of any disorder and incur a multitude of awful medical problems, including heart arrhythmia's (irregular heartbeats), kidney problems and osteoporosis. I would say I don't want to scare you, but I do; the risks of EDs are scary. The mortality rate for people with Anorexia is more than 5 times higher than the mortality rate for young females aged 15-34 in the general US population (Keshavia et al., 2014), 3% of people with Anorexia die from medical complications caused by starvation (Signorini et al., 2007), and many other individuals with Anorexia die from suicide (there is an 18 times higher risk of suicide in people with Anorexia according to Kashavia et al., 2014). Malnutrition also causes many other problems, including dry skin, downy hair on the arms, back, face, etc., yellowish tinge to the skin, over-sensitivity to the cold (including purplish extremities due to a lack of oxygen). Low blood pressure often causes individuals to feel dizzy and faint. Vitamin B deficiency is also a big risk and can lead to depression and cognitive changes often seen in people at low weights. One of the biggest and longest standing risks is osteoporosis; if you fail to eat properly during adolescence and early adulthood, when peak bone density should be achieved, you may suffer from weak/fragile bones for the rest of your life, even if you recover. Imbalances in electrolytes, including potassium, can lead to heart arrhythmia's which can be lethal. This is also a big risk in Bulimia, as purging through vomiting and/or laxatives can lead to imbalances in electrolytes. Chronically low potassium levels can lead to kidney damage and renal failure which may require dialysis. Laxative abuse can also cause gastrointestinal problems, damage to the bowels and dehydration. People with Bulimia may also end up with calluses on their hands from using their fingers to throw up, dental problems including cavities and mouth ulcers, and even tears of the throat caused by using objects to throw up. So it is clear how dangerous eating disorders can be, and although Bulimia has a lower mortality rate than Anorexia, people with Bulimia are still twice as likely to die than their non-Bulimic peers (Arceulus et al., 2011).
That's the bad news. The good news is that recovery is very possible! Lowe et al. (2001) found that, 21 years after first seeking treatment, 16% of Anorexic patients were no longer alive, 10% were still suffering, 21% had partially recovered and 51% had fully recovered. This is very promising as it suggests that, even though Anorexia is a very dangerous illness, it is still more likely for people to get better than to not get better. Furthermore, Keel et al. (1999) and Fichter & Quadfleig (2007) found that, at the end of an 11-12 year follow-up, 70% of Bulimic patients were in remission, no longer meeting the criteria for any ED. The earlier an individual is given treatment, the more likely they are to recover. Arcelus (2011) found those who were older when first receiving treatment for Anorexia were more likely to die prematurely. I do not want to pretend that recovery is all rosy; recovery is subjective, and many people who no longer meet diagnostic criteria for an eating disorder still suffer from weight and body-shape concerns, as well as problems with food (Sullivan, 2002). Despite this, it is clear that it is very possible for someone who has suffered from an eating disorder to live a full and happy life. Things may never be the same again, I'm afraid, but they can still be wonderful, and beautiful, and worth fighting for. When I was ill I thought there was no way I could ever be okay, and that I'd end up in a ditch. I wouldn't have believed that a few years later I'd be a healthy weight, relatively happy with myself and enjoying my life. So, to anyone suffering from an ED, if I was able to do it, you definately can. It will not be easy, I won't lie, but it will be worth it. Living with an eating disorder is no way to live.
References and useful links:
Hooley et al. (2016) Abnormal Psychology
https://www.beateatingdisorders.org.uk/
NHS website: eating disorder section
NHS website: BMI calculator
Why mental health should be taken as seriously as physical health
Ever been told 'it's all in your mind', as though what you are feeling isn't real? Ever been made to feel like you're wasting hospital time/government services because you're being treated for mental health rather than something 'physical'? It can be very upsetting. Sometimes when you have a mental health problem you can feel like you're 'making something out of nothing' or that you're complaining self-indulgently while there are people who have 'real problems', especially when you get told to 'get over it'. The thing is, mental health is a big issue and it is serious. While physical health is, of course, very, very important, that doesn't mean that mental health isn't also as important. In fact, I'm going to argue that mental health is closely intertwined with physical health, and is a form of physical health in itself; the physical health of the brain. Furthermore, mental health effects physical health in many ways, and its often very difficult to maintain good physical health without good mental health.
There is much evidence that mental health problems are routed in brain abnormalities such as neurotransmitter deficiencies. Neurotransmitters are chemical substances in the brain that send messages from one neuron to another. These messages can be inhibitory (they prevent/reduce the activity of a neuron) or exitatory (they increase the activity of a neuron). Some neurotransmitters are abnormal in the brains of people with mental health problems. For example, many people with depression lack serotonin (a neruotransmitter involved in mood, appetite and sleep), and drugs that increase the amount of serotonin in the brain by blocking serotonin re-uptake (the process of returning serotonin back to the original neuron) are often very effective in treating depression. Furthermore, dopamine (a neurotransmitter involved in thought, movement and vision) is thought to be associated with schizophrenia; fMRI scans have suggested that those with schizophrenia have excess dopamine in their brains, which may be a cause of positive symptoms such as delusions and hallucinations, as well as catatonic/abnormal motor activity.
Another way in which mental health is similar to physical health is the effect it can have on the body. This is most starkly seen in eating disorders; people with eating disorders can badly damage their bodies through purging, binging and/or starving. For example, physical symptoms of Anorexia include dizziness, fine downy hair, very low weight, low potassium, dry skin, thin/brittle hair and this disorder can even lead to osteoporosis and heart problems. It is clear that eating disorders can be as much a physical health problem as a mental health problem, and the physical consequences of severe Anorexia often have to be treated first in order for the patient to improve their mental health. Mental health problems also often include many physical symptoms; anxiety often involves nausea, dizziness and heart palpitations, and people with the form of anxiety panic disorder (which involves frequent panic attacks and anticipatory anxiety surrounding a fear of having panic attacks) actually have increased risk of physical health problems, including heart disease. It is clear that mental health can be damaging to the body and should be taken seriously as potentially causing physical health problems.
Physical health problems can be very debilitating and can effect people's daily life and ability to work; and so can mental health problems. Individuals with schizophrenia are significantly more likely to be of lower socioeconomic status and to be homeless than other people (Neugebauer et al. 1980, as cited by Link, Dohrenwend & Skodol, 1987). Of course, directionality isn't established, but the social selection theory proposes that individuals with schizophrenia are unable to maintain jobs due to their disorder and so are unable to move up the social ladder and/or actually fall lower down the social ladder (Link, Dohrenwend & Skodol, 1987). Furthermore, part of the DSM (Diagnostic and Statistical Manual for Mental Disorders) criteria for schizophrenia is that a patient should have experienced significant impairment in areas including occupational and social functioning. This shows how debilitating mental health can be. Many mental health problems are only considered problems for this very reason; they significantly and negatively impact people's lives. Since mental health problems can cause so much distress and impairment, it seems obvious that they should be taken seriously.
Physical health and mental health are very intertwined; people with poor physical health often also suffer from mental health problems, especially depression. For example, people with Psoriasis (an auto-immune condition) are vulnerable to depression and anxiety; 1 third report experiencing depression and anxiety (https://www.mentalhealth.org.uk/a-to-z/p/physical-health-and-mental-health). Considering how clearly linked physical and mental health is, it seems odd to take one of them more seriously than the other. I therefore urge people to consider their mental and physical health as both important and vital parts of their overall wellbeing, and to take those with mental health problems as seriously as those with physical health problems.
References and useful links:
https://link.springer.com/chapter/10.1007/978-3-642-52057-0_5#citeas
https://www.mentalhealth.org.uk/a-to-z/p/physical-health-and-mental-health
Ever been told 'it's all in your mind', as though what you are feeling isn't real? Ever been made to feel like you're wasting hospital time/government services because you're being treated for mental health rather than something 'physical'? It can be very upsetting. Sometimes when you have a mental health problem you can feel like you're 'making something out of nothing' or that you're complaining self-indulgently while there are people who have 'real problems', especially when you get told to 'get over it'. The thing is, mental health is a big issue and it is serious. While physical health is, of course, very, very important, that doesn't mean that mental health isn't also as important. In fact, I'm going to argue that mental health is closely intertwined with physical health, and is a form of physical health in itself; the physical health of the brain. Furthermore, mental health effects physical health in many ways, and its often very difficult to maintain good physical health without good mental health.
There is much evidence that mental health problems are routed in brain abnormalities such as neurotransmitter deficiencies. Neurotransmitters are chemical substances in the brain that send messages from one neuron to another. These messages can be inhibitory (they prevent/reduce the activity of a neuron) or exitatory (they increase the activity of a neuron). Some neurotransmitters are abnormal in the brains of people with mental health problems. For example, many people with depression lack serotonin (a neruotransmitter involved in mood, appetite and sleep), and drugs that increase the amount of serotonin in the brain by blocking serotonin re-uptake (the process of returning serotonin back to the original neuron) are often very effective in treating depression. Furthermore, dopamine (a neurotransmitter involved in thought, movement and vision) is thought to be associated with schizophrenia; fMRI scans have suggested that those with schizophrenia have excess dopamine in their brains, which may be a cause of positive symptoms such as delusions and hallucinations, as well as catatonic/abnormal motor activity.
Another way in which mental health is similar to physical health is the effect it can have on the body. This is most starkly seen in eating disorders; people with eating disorders can badly damage their bodies through purging, binging and/or starving. For example, physical symptoms of Anorexia include dizziness, fine downy hair, very low weight, low potassium, dry skin, thin/brittle hair and this disorder can even lead to osteoporosis and heart problems. It is clear that eating disorders can be as much a physical health problem as a mental health problem, and the physical consequences of severe Anorexia often have to be treated first in order for the patient to improve their mental health. Mental health problems also often include many physical symptoms; anxiety often involves nausea, dizziness and heart palpitations, and people with the form of anxiety panic disorder (which involves frequent panic attacks and anticipatory anxiety surrounding a fear of having panic attacks) actually have increased risk of physical health problems, including heart disease. It is clear that mental health can be damaging to the body and should be taken seriously as potentially causing physical health problems.
Physical health problems can be very debilitating and can effect people's daily life and ability to work; and so can mental health problems. Individuals with schizophrenia are significantly more likely to be of lower socioeconomic status and to be homeless than other people (Neugebauer et al. 1980, as cited by Link, Dohrenwend & Skodol, 1987). Of course, directionality isn't established, but the social selection theory proposes that individuals with schizophrenia are unable to maintain jobs due to their disorder and so are unable to move up the social ladder and/or actually fall lower down the social ladder (Link, Dohrenwend & Skodol, 1987). Furthermore, part of the DSM (Diagnostic and Statistical Manual for Mental Disorders) criteria for schizophrenia is that a patient should have experienced significant impairment in areas including occupational and social functioning. This shows how debilitating mental health can be. Many mental health problems are only considered problems for this very reason; they significantly and negatively impact people's lives. Since mental health problems can cause so much distress and impairment, it seems obvious that they should be taken seriously.
Physical health and mental health are very intertwined; people with poor physical health often also suffer from mental health problems, especially depression. For example, people with Psoriasis (an auto-immune condition) are vulnerable to depression and anxiety; 1 third report experiencing depression and anxiety (https://www.mentalhealth.org.uk/a-to-z/p/physical-health-and-mental-health). Considering how clearly linked physical and mental health is, it seems odd to take one of them more seriously than the other. I therefore urge people to consider their mental and physical health as both important and vital parts of their overall wellbeing, and to take those with mental health problems as seriously as those with physical health problems.
References and useful links:
https://link.springer.com/chapter/10.1007/978-3-642-52057-0_5#citeas
https://www.mentalhealth.org.uk/a-to-z/p/physical-health-and-mental-health

Should there be a weight criterion for Anorexia Nervosa?
Did you know that the only difference between the binging/purging subtype of Anorexia Nervosa (AN) and Bulimia Nervosa (BN) is weight? What this means is that if someone with BN loses weight, they will be reclassified as having AN binging/purging subtype, and if someone with this subtype of AN gains weight, they will be reclassified as having BN. I'm going to run through a couple of arguments for why this might be problematic, and also why it might be necessary.
Firstly, no other mental disorder is classified in terms of physical attributes; they are all classified in terms of a set of psychological, behavioural and emotional traits/characteristics. AN is the only mental disorder that has a physical requirement, and the only eating disorder (ED) that has a weight requirement. One problem with this is that the criterion in itself might not be valid. For example, Watson & Andersen (2003) compared individuals with AN to those who had the same psychopathology and self-starvation but didn’t meet the AN criteria of weight loss below 15% of healthy weight. These people were classified as having ‘atypical’ anorexia or an Eating Disorder Not Otherwise Specified (EDNOS). However, there were no differences in demographics, illness history, treatment response, psychopathology or bone density (Watson & Andersen, 2003). If there is no psychological/behavioural difference between individuals who are diagnosed as having AN and those who have all the symptoms but low weight, then it seems reasonable to conclude that the weight criterion for AN might not be very good.
Secondly, those who are diagnosed with AN tend to have poorer prospects than those diagnosed with BN or BED. This should be investigated further because it could be that those who have BN and are able to maintain a healthy weight are better able to respond to treatment because of their higher weight (which often aids in recovery by allowing people to think more clearly) or they respond better to treatment and so are able to maintain a healthy weight. Furthermore, those who have AN and then gain weight might do this because they are recovering, and so probably shouldn't be reclassified as having BN, but should be thought of as being in a different stage of their illness. Some researchers have argued that the AN binging/purging subtype should actually be considered a form of BN (Hooley et al., 2016) and there is good reason to think that AN and BN are very closely linked. The psychological symptoms of both disorders are very similar. For example, people with BN and AN both experience concerns around weight and food, fears of gaining weight and body image issues. Furthermore, people with AN restricting subtype often change to having AN binging/purging subtype and sometimes then to BN (Hooley et al., 2013). Given the common diagnostic crossover between the two disorders, it could be that they are actually part of the same underlying psychological condition, and should therefore be treated the same.
This links in to my third point; doctors often treat patients in terms of weight when it comes to ED's. I, for example, was discharged when I reached a healthy weight, despite still struggling with my thoughts and emotions around food. While it is important to make sure patients reach and maintain a healthy weight, I feel that people with BN or atypical AN who are at a healthy weight are often not taken as seriously as those who are underweight. This is problematic because people who are at a healthy weight with BN can still be putting their lives at risk; frequent vomiting can lead to low potassium which can increase the risk of heart failure. Furthermore, some people with AN may have started restricting their eating at a high weight, and so may have lost a very significant amount of weight already even if they are at a technically healthy weight. Losing a lot of weight in a short amount of time through unhealthy methods is dangerous, and can cause damage to the body, including the heart and metabolic systems, even if a person is at a healthy weight. For these reasons I think it's a shame that weight is often the top priority for doctors when it comes to EDs.
However, even though individuals with EDs who are at a healthy weight can still be in danger, I do not want to overlook how dangerous being significantly underweight is. For example, it can cause osteoporosis (weak bones), heart failure, hair loss, dizziness, (Hooley et al., 2016) and even death. In fact, the mortality rate for AN has been estimated to be at around 16% (Lowe et al., 2001, as cited by Hooley et al., 2016), and AN has the highest mortality rate of any mental disorder. Self-starvation is something that will kill a person eventually if they do not get help. For this reason, having a weight criterion for AN might be necessary as it allows doctors to recognise those patients who are at most immediate physical risk, and who are most likely to require intensive inpatient treatment. For this reason, I do not totally discredit the weight criterion for AN, but I would suggest seperating the psychological diagnosis of AN from any physical diagnoses like low BMI. It might be beneficial to monitor the physical condition of patients with all EDs alongside monitoring their psychological wellbeing. This would mean that individuals at healthy weights who are also at physical risk won't be missed.
So, in conclusion, there are arguments for and against the weight criterion of AN, and if you're interested and want to know more you might want to take a look at the NHS website or type in Anorexia and weight into google scholar; there are some good articles on the topic (also check out the references at the bottom).
References:
Hooley M., J., Butcher N., J., Nock, K., M., Mineka, S (2016). Abnormal Psychology, Global Edition. Edinburgh Gate, Harlow, Essex: Pearson Education M.U.A.
Watson, T. L. and Andersen, A. E. (2003), A critical examination of the amenorrhea and weight criteria for diagnosing anorexia nervosa. Acta Psychiatrica Scandinavica, 108, 175–182.
Did you know that the only difference between the binging/purging subtype of Anorexia Nervosa (AN) and Bulimia Nervosa (BN) is weight? What this means is that if someone with BN loses weight, they will be reclassified as having AN binging/purging subtype, and if someone with this subtype of AN gains weight, they will be reclassified as having BN. I'm going to run through a couple of arguments for why this might be problematic, and also why it might be necessary.
Firstly, no other mental disorder is classified in terms of physical attributes; they are all classified in terms of a set of psychological, behavioural and emotional traits/characteristics. AN is the only mental disorder that has a physical requirement, and the only eating disorder (ED) that has a weight requirement. One problem with this is that the criterion in itself might not be valid. For example, Watson & Andersen (2003) compared individuals with AN to those who had the same psychopathology and self-starvation but didn’t meet the AN criteria of weight loss below 15% of healthy weight. These people were classified as having ‘atypical’ anorexia or an Eating Disorder Not Otherwise Specified (EDNOS). However, there were no differences in demographics, illness history, treatment response, psychopathology or bone density (Watson & Andersen, 2003). If there is no psychological/behavioural difference between individuals who are diagnosed as having AN and those who have all the symptoms but low weight, then it seems reasonable to conclude that the weight criterion for AN might not be very good.
Secondly, those who are diagnosed with AN tend to have poorer prospects than those diagnosed with BN or BED. This should be investigated further because it could be that those who have BN and are able to maintain a healthy weight are better able to respond to treatment because of their higher weight (which often aids in recovery by allowing people to think more clearly) or they respond better to treatment and so are able to maintain a healthy weight. Furthermore, those who have AN and then gain weight might do this because they are recovering, and so probably shouldn't be reclassified as having BN, but should be thought of as being in a different stage of their illness. Some researchers have argued that the AN binging/purging subtype should actually be considered a form of BN (Hooley et al., 2016) and there is good reason to think that AN and BN are very closely linked. The psychological symptoms of both disorders are very similar. For example, people with BN and AN both experience concerns around weight and food, fears of gaining weight and body image issues. Furthermore, people with AN restricting subtype often change to having AN binging/purging subtype and sometimes then to BN (Hooley et al., 2013). Given the common diagnostic crossover between the two disorders, it could be that they are actually part of the same underlying psychological condition, and should therefore be treated the same.
This links in to my third point; doctors often treat patients in terms of weight when it comes to ED's. I, for example, was discharged when I reached a healthy weight, despite still struggling with my thoughts and emotions around food. While it is important to make sure patients reach and maintain a healthy weight, I feel that people with BN or atypical AN who are at a healthy weight are often not taken as seriously as those who are underweight. This is problematic because people who are at a healthy weight with BN can still be putting their lives at risk; frequent vomiting can lead to low potassium which can increase the risk of heart failure. Furthermore, some people with AN may have started restricting their eating at a high weight, and so may have lost a very significant amount of weight already even if they are at a technically healthy weight. Losing a lot of weight in a short amount of time through unhealthy methods is dangerous, and can cause damage to the body, including the heart and metabolic systems, even if a person is at a healthy weight. For these reasons I think it's a shame that weight is often the top priority for doctors when it comes to EDs.
However, even though individuals with EDs who are at a healthy weight can still be in danger, I do not want to overlook how dangerous being significantly underweight is. For example, it can cause osteoporosis (weak bones), heart failure, hair loss, dizziness, (Hooley et al., 2016) and even death. In fact, the mortality rate for AN has been estimated to be at around 16% (Lowe et al., 2001, as cited by Hooley et al., 2016), and AN has the highest mortality rate of any mental disorder. Self-starvation is something that will kill a person eventually if they do not get help. For this reason, having a weight criterion for AN might be necessary as it allows doctors to recognise those patients who are at most immediate physical risk, and who are most likely to require intensive inpatient treatment. For this reason, I do not totally discredit the weight criterion for AN, but I would suggest seperating the psychological diagnosis of AN from any physical diagnoses like low BMI. It might be beneficial to monitor the physical condition of patients with all EDs alongside monitoring their psychological wellbeing. This would mean that individuals at healthy weights who are also at physical risk won't be missed.
So, in conclusion, there are arguments for and against the weight criterion of AN, and if you're interested and want to know more you might want to take a look at the NHS website or type in Anorexia and weight into google scholar; there are some good articles on the topic (also check out the references at the bottom).
References:
Hooley M., J., Butcher N., J., Nock, K., M., Mineka, S (2016). Abnormal Psychology, Global Edition. Edinburgh Gate, Harlow, Essex: Pearson Education M.U.A.
Watson, T. L. and Andersen, A. E. (2003), A critical examination of the amenorrhea and weight criteria for diagnosing anorexia nervosa. Acta Psychiatrica Scandinavica, 108, 175–182.
Self-medicating vs. Medicine
Self-medicating involves taking drugs/alcohol in order to control one's mood. For example, if you are struggling to sleep you might drink to help, if you're feeling low you might take a psychoactive drug such as Marijuana to lift your mood. Self-medicating is common in Bipolar Disorder as well as other mental illnesses, as well as in people without a diagnosed condition who are trying to cope with stress. One reason a person might start self-medicating is through taking drugs/alcohol recreationally, and finding them useful for coping with distressing thoughts/feelings in the short-term. However, short-term recreational use can often turn into long-term addictions and tends to be ineffective for actual recovery from mental health problems. For example, people who deal with depressive symptoms by drinking often become alcoholic and reliant on drink to get through the day. Another down-side of self-medicating is that some substances, such as Marijuana, have been linked to increased risk of mental health problems in people who are already at risk. This means that using weed as a coping mechanism for a mental health problem, whilst relieving in the short-term, may exacerbate the problem in the long-term. The reason that self-medicating often doesn't work is that the way it works on the brain is different to pharmacological medication; it changes brain chemistry in the short term and is often addictive, for example, alcohol increases GABA (an inhibitory neurotransmitter), leaving you feeling less inhibited and eventually shutting down brain functions, such as higher cognitive processing. This is only temporary, and even though it can calm down feelings of anxiety and restlessness, it won't change any faulty brain-chemistry which may be the underlying cause of a mental health problem. Furthermore, alcohol involves an increasing amount of tolerance the more it is used, meaning that after a while, a person will need more units of alcohol in order to get the same feelings of intoxication. For these reasons, a person who becomes dependent on alcohol will not be able to solve their anxiety problem, but will simply require alcohol to keep themselves functioning and avoid withdrawal symptoms. While recreational drugs and alcohol aren't inherently bad, it's good to make sure that, if you have signs of a mental health problem, you're being careful with them, and that if you begin to use them to cope with emotions and stress, you try to cut down/stop. Another reason why self-medication is not a good route to go down is that it can actually increase mental health problems. For example, marijuana can increase anxiety. And, as my girlfriend points out, alcohol can make you do things you wouldn't do sober, which can lead to feelings of guilt, which can then worsen depressive feelings. Furthermore, the money you spend on drugs/alcohol can sometimes lead to financial problems, adding an extra stress that you definately don't need.
Medications you may be prescribed by a doctor fall into four main categories; anxiolytics (anti-anxiety), anti-depressants, anti-manics and anti-psychotics. Most anti-depressants work by inhibiting the reuptake of the neurotransmitter serotonin. This neurotransmitter has been linked to mood, appetite and sleep, and is often found to be lacking in people with depression. By blocking the reuptake of serotonin, anti-depressants cause there to be more serotonin in the brain, often alleviating the symptoms of depression within a few weeks. While anti-depressants work for many patients, one downside of these medications is that they have some unpleasant side-effects, such as nausea, headaches, and even suicidal thoughts (but these are rare). If you require anti-depressant medication your doctor will monitor you as you use it and change your medication/dose according to how you are feeling.
Anti-anxiety medications often work by slowing down the nervous system (Benzodiazepines), and the only long-term specifically anti-anxiety medication is Buspirone (Psych Central). Anti-psychotic medications often work by blocking Dopamine; this neurotransmitter has been found to be increased in people with disorders such as Schizophrenia and is involved in perception and motor movement, as well reward. It is believed that an increase in Dopamine is the cause of the positive (things that Schizophrenic people have and others don't have) symptoms of Schizophrenia, e.g. hallucinations and delusions. Dopamine may also be responsible for the negative symptoms (things people with Schizophrenia lack), such as catatonic movements (being very still) and flat affect (lack of emotion), but since Dopamine blocking medication is rarely effective for the negative symptoms (things people with Schizophrenia lack), it is likely that Dopamine isn't the main cause of these. D2 (Dopamine) antagonists are thought to be the only truly effective treatment for Schizophrenia and work by blocking Dopamine (Martin et al., 2013. A problem with D2 antagonists is that, because they don't discriminate between the different Dopamine systems (one is involved in movement, the other in perception and reward), when someone takes these antipsychotic medications they can suffer from movement disorders, such as tardive dyskinesia, involving involuntary lip-smacking and drooling (Martin et al., 2013). Lithium is a common anti-manic drug; it is a mood stabilizer often used to treat Bipolar Disorder. All of these drugs have up-sides and down-sides, so you should make sure that you are fully informed before you make a decision, and that you take into account the doctors advice. A benefit of drug treatment is that these treatments are often effective in reducing/managing symptoms of mental health problems. However, some critics argue that drug treatments don't deal with the underlying issues which cause mental health probelms, such as distorted thinking and stressful life events, and so aren't really effective in treating mental illness. Furthermore, psychological treatments, such as CBT, have been found to be just as, if not more, effective than drug treatments. Most of the time treatment for mental health problems involves both psychological and pharmacological treatments, so if you go to your GP for help with something such as depression, you will most likely be prescribed an antidepressant and also be referred for some kind of psychological therapy. Remember that if a medication is not working for you, or the side-effects are too much to deal with, you should talk to your doctor straight away and get it changed. Most importantly, remember that doctors want to help you and won't prescribe anything they don't feel is necessary.
Self-medicating involves taking drugs/alcohol in order to control one's mood. For example, if you are struggling to sleep you might drink to help, if you're feeling low you might take a psychoactive drug such as Marijuana to lift your mood. Self-medicating is common in Bipolar Disorder as well as other mental illnesses, as well as in people without a diagnosed condition who are trying to cope with stress. One reason a person might start self-medicating is through taking drugs/alcohol recreationally, and finding them useful for coping with distressing thoughts/feelings in the short-term. However, short-term recreational use can often turn into long-term addictions and tends to be ineffective for actual recovery from mental health problems. For example, people who deal with depressive symptoms by drinking often become alcoholic and reliant on drink to get through the day. Another down-side of self-medicating is that some substances, such as Marijuana, have been linked to increased risk of mental health problems in people who are already at risk. This means that using weed as a coping mechanism for a mental health problem, whilst relieving in the short-term, may exacerbate the problem in the long-term. The reason that self-medicating often doesn't work is that the way it works on the brain is different to pharmacological medication; it changes brain chemistry in the short term and is often addictive, for example, alcohol increases GABA (an inhibitory neurotransmitter), leaving you feeling less inhibited and eventually shutting down brain functions, such as higher cognitive processing. This is only temporary, and even though it can calm down feelings of anxiety and restlessness, it won't change any faulty brain-chemistry which may be the underlying cause of a mental health problem. Furthermore, alcohol involves an increasing amount of tolerance the more it is used, meaning that after a while, a person will need more units of alcohol in order to get the same feelings of intoxication. For these reasons, a person who becomes dependent on alcohol will not be able to solve their anxiety problem, but will simply require alcohol to keep themselves functioning and avoid withdrawal symptoms. While recreational drugs and alcohol aren't inherently bad, it's good to make sure that, if you have signs of a mental health problem, you're being careful with them, and that if you begin to use them to cope with emotions and stress, you try to cut down/stop. Another reason why self-medication is not a good route to go down is that it can actually increase mental health problems. For example, marijuana can increase anxiety. And, as my girlfriend points out, alcohol can make you do things you wouldn't do sober, which can lead to feelings of guilt, which can then worsen depressive feelings. Furthermore, the money you spend on drugs/alcohol can sometimes lead to financial problems, adding an extra stress that you definately don't need.
Medications you may be prescribed by a doctor fall into four main categories; anxiolytics (anti-anxiety), anti-depressants, anti-manics and anti-psychotics. Most anti-depressants work by inhibiting the reuptake of the neurotransmitter serotonin. This neurotransmitter has been linked to mood, appetite and sleep, and is often found to be lacking in people with depression. By blocking the reuptake of serotonin, anti-depressants cause there to be more serotonin in the brain, often alleviating the symptoms of depression within a few weeks. While anti-depressants work for many patients, one downside of these medications is that they have some unpleasant side-effects, such as nausea, headaches, and even suicidal thoughts (but these are rare). If you require anti-depressant medication your doctor will monitor you as you use it and change your medication/dose according to how you are feeling.
Anti-anxiety medications often work by slowing down the nervous system (Benzodiazepines), and the only long-term specifically anti-anxiety medication is Buspirone (Psych Central). Anti-psychotic medications often work by blocking Dopamine; this neurotransmitter has been found to be increased in people with disorders such as Schizophrenia and is involved in perception and motor movement, as well reward. It is believed that an increase in Dopamine is the cause of the positive (things that Schizophrenic people have and others don't have) symptoms of Schizophrenia, e.g. hallucinations and delusions. Dopamine may also be responsible for the negative symptoms (things people with Schizophrenia lack), such as catatonic movements (being very still) and flat affect (lack of emotion), but since Dopamine blocking medication is rarely effective for the negative symptoms (things people with Schizophrenia lack), it is likely that Dopamine isn't the main cause of these. D2 (Dopamine) antagonists are thought to be the only truly effective treatment for Schizophrenia and work by blocking Dopamine (Martin et al., 2013. A problem with D2 antagonists is that, because they don't discriminate between the different Dopamine systems (one is involved in movement, the other in perception and reward), when someone takes these antipsychotic medications they can suffer from movement disorders, such as tardive dyskinesia, involving involuntary lip-smacking and drooling (Martin et al., 2013). Lithium is a common anti-manic drug; it is a mood stabilizer often used to treat Bipolar Disorder. All of these drugs have up-sides and down-sides, so you should make sure that you are fully informed before you make a decision, and that you take into account the doctors advice. A benefit of drug treatment is that these treatments are often effective in reducing/managing symptoms of mental health problems. However, some critics argue that drug treatments don't deal with the underlying issues which cause mental health probelms, such as distorted thinking and stressful life events, and so aren't really effective in treating mental illness. Furthermore, psychological treatments, such as CBT, have been found to be just as, if not more, effective than drug treatments. Most of the time treatment for mental health problems involves both psychological and pharmacological treatments, so if you go to your GP for help with something such as depression, you will most likely be prescribed an antidepressant and also be referred for some kind of psychological therapy. Remember that if a medication is not working for you, or the side-effects are too much to deal with, you should talk to your doctor straight away and get it changed. Most importantly, remember that doctors want to help you and won't prescribe anything they don't feel is necessary.
Body positivity: How to Achieve it
Being body positive is one of the hardest things you can do, especially if you have low self esteem or have suffered with an eating disorder. It's eating disorder awareness week, so I've decided to dedicate this article to those suffering with/recovering from eating disorders. However, the tips I'll be giving can be applied to anyone suffering from a lack of body positivity; everyone deserves to feel good about themselves.
Tip One: When gaining weight, please, for heavens sake, do not keep your old clothes. Having small sizes around which no longer fit you can serve as a motivation to lose weight and/or can make it harder to accept the changes to your body. You need to remember that if you are in recovery from a restrictive/purging eating disorder you will probably need to gain weight to be healthy, and so weight gain is a good thing for you; holding on to old clothes from when you were ill is no way to recover. This is also a great excuse to go shopping and treat yourself, which is an important step to feeling better (see tip four).
Tip Two: Do not, I repeat not, have images of skinny women/overly muscular men or any pictures which will make you feel bad about your body. I know how tempting it can be to reach into the depths of the internet and find thinspiration, but you won't feel body positive if your looking at people who have unrealistic/emancipated bodies. It's a good idea to have images of people with all different kinds of bodies; it can remind you that everyone is beautiful in their own way. Don't let yourself get sucked in by the 'thin' ideal of magazines and a lot of TV shows; it's just not healthy. This may also require boycotting certain TV shows, especially dieting shows (for the purposes of recovery, these are the devil).
Tip Three: Remember that food is fuel; use it to be healthy, not to control your body. Try to eat healthily, have lots of fruit and veg, but also let yourself have treats, and do NOT let yourself go hungry. Listen to your body; humans have evolved for billions of years, our stomachs know what they're talking about! Try to think of food as your friend, as something that is there to keep your body working properly, like petrol in a car. It's not there to make you lose or gain weight. It can be really tempting to think of foods in terms of calories, fat and carbs, but that isn't healthy or helpful for recovery, or for feeling good about yourself. The more you focus on how many calories you're eating, the more likely it is that you'll start to fall into unhealthy habits and feel anxious about your body.
Tip Four: Treat yourself- this can be very difficult for someone with low self-esteem and/or who's recovering from an eating disorder, but it is very important. When you don't feel good about yourself it can be easy to neglect your body and your mind; you might not think you deserve to go shopping and get nice things, or to do the things that make you happy, or be pampered, but that's what you deserve more than anything. Have a nice bubble bath, paint your nails, get your hair done, watch your favorite movie; do something to treat yourself. Being able ot be nice to yourself is one of the most important steps to recovering from low self-esteem and achieving body positivity; how can you love your body if you're not willing to treat it? If you find this difficult, it might be helpful to think of it as treating yourself like you'd treat your best friend.
Tip Five: Learn your body. A good thing to do is sit in front of the mirror naked and just look at your body without judgement. This is very difficult and can take a lot of practice, but once you're able to do this, you will feel better about your body. Learn how many rolls your stomach has, how many spots or freckles there are on your skin. Once you can do this without judging yourself, you need to be able to say nice things about your body. There will be something, whether it's your eyes or your hair or your fingernails, you will find something. Being able to just look at and accept your body is a very difficult skill, but it's a very powerful way of gaining body positivity, so try it!
Tip Six: Surround yourself with positivity- look for body positive images on Tumblr and Pintrest, listen to TED talks like https://www.youtube.com/watch?v=LSMH3WABkwg, cover your walls with pictures of plus sized models and people of all different sizes. Say at least five nice things about yourself every morning; even if you don't believe them at first, they'll eventually sink in.
These are just a few tips on improving self-esteem and gaining body positivity which I have found helpful. If you are suffering from very low self-esteem or have an untreated eating disorder you should talk to your GP to get help.
Resources:
https://www.beateatingdisorders.org.uk/
https://youngminds.org.uk/
Being body positive is one of the hardest things you can do, especially if you have low self esteem or have suffered with an eating disorder. It's eating disorder awareness week, so I've decided to dedicate this article to those suffering with/recovering from eating disorders. However, the tips I'll be giving can be applied to anyone suffering from a lack of body positivity; everyone deserves to feel good about themselves.
Tip One: When gaining weight, please, for heavens sake, do not keep your old clothes. Having small sizes around which no longer fit you can serve as a motivation to lose weight and/or can make it harder to accept the changes to your body. You need to remember that if you are in recovery from a restrictive/purging eating disorder you will probably need to gain weight to be healthy, and so weight gain is a good thing for you; holding on to old clothes from when you were ill is no way to recover. This is also a great excuse to go shopping and treat yourself, which is an important step to feeling better (see tip four).
Tip Two: Do not, I repeat not, have images of skinny women/overly muscular men or any pictures which will make you feel bad about your body. I know how tempting it can be to reach into the depths of the internet and find thinspiration, but you won't feel body positive if your looking at people who have unrealistic/emancipated bodies. It's a good idea to have images of people with all different kinds of bodies; it can remind you that everyone is beautiful in their own way. Don't let yourself get sucked in by the 'thin' ideal of magazines and a lot of TV shows; it's just not healthy. This may also require boycotting certain TV shows, especially dieting shows (for the purposes of recovery, these are the devil).
Tip Three: Remember that food is fuel; use it to be healthy, not to control your body. Try to eat healthily, have lots of fruit and veg, but also let yourself have treats, and do NOT let yourself go hungry. Listen to your body; humans have evolved for billions of years, our stomachs know what they're talking about! Try to think of food as your friend, as something that is there to keep your body working properly, like petrol in a car. It's not there to make you lose or gain weight. It can be really tempting to think of foods in terms of calories, fat and carbs, but that isn't healthy or helpful for recovery, or for feeling good about yourself. The more you focus on how many calories you're eating, the more likely it is that you'll start to fall into unhealthy habits and feel anxious about your body.
Tip Four: Treat yourself- this can be very difficult for someone with low self-esteem and/or who's recovering from an eating disorder, but it is very important. When you don't feel good about yourself it can be easy to neglect your body and your mind; you might not think you deserve to go shopping and get nice things, or to do the things that make you happy, or be pampered, but that's what you deserve more than anything. Have a nice bubble bath, paint your nails, get your hair done, watch your favorite movie; do something to treat yourself. Being able ot be nice to yourself is one of the most important steps to recovering from low self-esteem and achieving body positivity; how can you love your body if you're not willing to treat it? If you find this difficult, it might be helpful to think of it as treating yourself like you'd treat your best friend.
Tip Five: Learn your body. A good thing to do is sit in front of the mirror naked and just look at your body without judgement. This is very difficult and can take a lot of practice, but once you're able to do this, you will feel better about your body. Learn how many rolls your stomach has, how many spots or freckles there are on your skin. Once you can do this without judging yourself, you need to be able to say nice things about your body. There will be something, whether it's your eyes or your hair or your fingernails, you will find something. Being able to just look at and accept your body is a very difficult skill, but it's a very powerful way of gaining body positivity, so try it!
Tip Six: Surround yourself with positivity- look for body positive images on Tumblr and Pintrest, listen to TED talks like https://www.youtube.com/watch?v=LSMH3WABkwg, cover your walls with pictures of plus sized models and people of all different sizes. Say at least five nice things about yourself every morning; even if you don't believe them at first, they'll eventually sink in.
These are just a few tips on improving self-esteem and gaining body positivity which I have found helpful. If you are suffering from very low self-esteem or have an untreated eating disorder you should talk to your GP to get help.
Resources:
https://www.beateatingdisorders.org.uk/
https://youngminds.org.uk/

Body Positivity: Why it's hard
It can be hard to be positive about your own body, especially when we see 'perfect' images all over the media. When I typed in top actress 2017 I was presented with a list of the hottest actresses. All of the women (Alexandra Daddario, Chloe Grace Moretz, Emmy Rossum, Hailee Steinfeld, Emma Roberts, Margot Robbie, Scarlet Johnson, Imogen Poots, Amber Heard and Francia Raisa) are undoubtedly beautiful. They're also very talented, and should be looked up to for more than their looks. There seems to be a trend in society, where women and girls are noticed much more for their looks than their achievements, even Hillary Clinton was mocked for 'looking old'. I noticed that all of the hottest actresses were conventionally beautiful; slim, mostly blonde, without a blemish. The problem is, most women just don't look like that. That can make us feel pretty bad about ourselves. According to the National Report on Self-Esteem, 98% of girls feel there is an immense pressure from external sources to look a certain way (National Report on Self Esteem) and 92% of teen girls would like to change something about the way they look, with body weight ranking the highest. (Dove campaign). Perhaps more alarmingly, 1 in 4 girls fall into a clinical category such as self-harm, eating disorders, depression and/or anxiety (http://www.heartofleadership.org/statistics/). So, apparently, a lot of young girls are suffering with very low self-esteem and mental health problems. Many boys and men experience this too, but it's not clear what the exact numbers are, since many boys and men do not come forward with mental health difficulties. It's clear that there is a problem with body positivity for many people, and this is a dreadful shame. Low self-esteem is linked with depression and eating disorders (although causality is not established, and it's possible low self-esteem results from such disorders, rather than causing them). In my own experience, I know that, even if low self-esteem doesn't cause disorders, it can definitely maintain them. Having a problem such as an eating disorder, and having ready (and sometimes unwanted) access to images of very thin girls in magazines and on television, can make things worse. Of course, the media is not a devil, and it doesn't directly cause low self-esteem and eating disorders. However, it can perpetuate an unrealistic ideal, and represent it as the norm. For example, dieting adverts are almost always directed towards women, and the women shown in these adverts are almost always a normal weight. For example, this advert for slimfast-
So, basically, this woman is slim. She's probably at the low end of a healthy weight, certainly not overweight and certainly not in need of losing any weight. But her body shape/weight is what's being associated with dieting. It just seems a little...well, fucked up. If dieting is seen as a completely normal thing for women of a healthy weight to do, then how could be expect our sons and daughters to realise the danger of fad diets and losing a lot of weight in a short amount of time? Like losing electrolytes, malnutrition, dehydration and more (image and risks of weight loss sourced from: https://www.about-face.org/slim-fast-says-quick-fix-weight-loss-is-best/).
It can be hard to be positive about your own body, especially when we see 'perfect' images all over the media. When I typed in top actress 2017 I was presented with a list of the hottest actresses. All of the women (Alexandra Daddario, Chloe Grace Moretz, Emmy Rossum, Hailee Steinfeld, Emma Roberts, Margot Robbie, Scarlet Johnson, Imogen Poots, Amber Heard and Francia Raisa) are undoubtedly beautiful. They're also very talented, and should be looked up to for more than their looks. There seems to be a trend in society, where women and girls are noticed much more for their looks than their achievements, even Hillary Clinton was mocked for 'looking old'. I noticed that all of the hottest actresses were conventionally beautiful; slim, mostly blonde, without a blemish. The problem is, most women just don't look like that. That can make us feel pretty bad about ourselves. According to the National Report on Self-Esteem, 98% of girls feel there is an immense pressure from external sources to look a certain way (National Report on Self Esteem) and 92% of teen girls would like to change something about the way they look, with body weight ranking the highest. (Dove campaign). Perhaps more alarmingly, 1 in 4 girls fall into a clinical category such as self-harm, eating disorders, depression and/or anxiety (http://www.heartofleadership.org/statistics/). So, apparently, a lot of young girls are suffering with very low self-esteem and mental health problems. Many boys and men experience this too, but it's not clear what the exact numbers are, since many boys and men do not come forward with mental health difficulties. It's clear that there is a problem with body positivity for many people, and this is a dreadful shame. Low self-esteem is linked with depression and eating disorders (although causality is not established, and it's possible low self-esteem results from such disorders, rather than causing them). In my own experience, I know that, even if low self-esteem doesn't cause disorders, it can definitely maintain them. Having a problem such as an eating disorder, and having ready (and sometimes unwanted) access to images of very thin girls in magazines and on television, can make things worse. Of course, the media is not a devil, and it doesn't directly cause low self-esteem and eating disorders. However, it can perpetuate an unrealistic ideal, and represent it as the norm. For example, dieting adverts are almost always directed towards women, and the women shown in these adverts are almost always a normal weight. For example, this advert for slimfast-
So, basically, this woman is slim. She's probably at the low end of a healthy weight, certainly not overweight and certainly not in need of losing any weight. But her body shape/weight is what's being associated with dieting. It just seems a little...well, fucked up. If dieting is seen as a completely normal thing for women of a healthy weight to do, then how could be expect our sons and daughters to realise the danger of fad diets and losing a lot of weight in a short amount of time? Like losing electrolytes, malnutrition, dehydration and more (image and risks of weight loss sourced from: https://www.about-face.org/slim-fast-says-quick-fix-weight-loss-is-best/).
Another problem is the lack of actual plus-sized models. For example, Calvin Klein's first 'plus sized' model is a size 10. There are some amazing examples of plus sized models, and Myla Dalbesio is a beautiful model who does good work. It is nice to see a normal sized woman being a model, but it's also kind of disheartening that she's considered plus-sized. When we live in a society where the average woman is the same size as a 'plus sized' model, we end up with a society where the average woman feels too big. This is a great buisness tactic for the dieting industry, but not so good for women's self-esteem.
So, we've established that there's a lot of barriers in the way of women having good self-esteem which come from the media. Let's talk about the lads. I think you guys don't have as much of a problem when it comes to body image, although there is undoubtedly pressure to have muscles and be hot enough to get girls. There's also underdog guys, like Scott Pilgrim (Scott Pilgrim vs. the world) and Columbus (Zombieland) who are likable, intelligent and usually end up getting the girl. There's not really a female equivalent of that, so men know that they can be funny and charming and that's often enough, but girls know that if they're not also beautiful they're just not good enough. However, men have other problems which are just as damaging. There's an expectation that men will be tough and will not be emotional, with "man up" and "don't be a pussy" being among a couple of the many insults used to emasculate men for showing emotion. This deprives men from being able to open up about their emotions, and can even prevent some boys and men from seeking help for mental health problems. Speaking of which, there's a stereotype that only girls get eating disorders. While eating disorders are more common in girls, many boys also suffer, and are often overlooked due to the expectation that they couldn't have an eating disorder because they're a boy. So I do not want to overlook men's self-esteem, and I want to ensure that I address everyone, because self-esteem is important for everyone.
A problem with self-esteem in our society is that it tends to be linked to appearance. If a man doesn't look 'attractive', he better be very intelligent or very funny, and if a girl isn't attractive, she's just not as good as the 'pretty girls', no matter what she does. There have been some amazing campaigns to help tackle low-self esteem and body image problems. For example, Dove's capaign 'the evolution of a model' nicely demonstrates how many of the images we see of women are extensively photoshopped and do not even look like the models in the photo, let alone the average woman. This distorts the perception of what is attainable, and also of what is normal. When we are encouraged to strive for an unattainable ideal, we're obviously going to become dissapointed with ourselves. It's as though we've been given the goal of creating a perfect world, it just won't happen. Most people will not be able to look like models, most models don't look like models in real life. But everyone deserves to feel good about themselves, and everyone is beautiful is their own way. Instead of trying to strive for an unattainable goal, I think we should strive to broaden the goal. Beautiful should include people of all sizes, ages, races and gender identities. Who decided that being a size 6 was beautiful? Why can't a size 16 also be beautiful?
Above and beyond the idea of aesthetics, why don't be think about weight in terms of health? I mean, that's the only reason anyone should ever really need to change their weight. If you're having health problems due to being overweight, it's beneficial to lose weight. If you're having health problems from being underweight, you should put on weight. But if you're not having any problems, and you're within a healthy weight range, why should you have to worry about your weight? Isn't it odd that physical appearance is often put above health? Another thing which is odd is the perception of people as vein if they like the way that they look. For example, the lyrics "you don't know you're beautiful, and that's what makes you beautiful" (1D, ugh I know, you don't know you're beautiful) seem to represent the pervasive idea that it's 'cute' or 'desirable' for someone (especially a girl) to be insecure. It really shouldn't be. There's nothing bad about a person who is insecure, but insecurity shouldn't be encouraged, it sucks. Not liking yourself can take your attention away from school/work, it can make you not want to leave the house, it can make you feel very low and is just not fun. So, I'm askng people to please just try and accept that it's okay to like yourself, you should aim to love yourself.
So, we've established that there's a lot of barriers in the way of women having good self-esteem which come from the media. Let's talk about the lads. I think you guys don't have as much of a problem when it comes to body image, although there is undoubtedly pressure to have muscles and be hot enough to get girls. There's also underdog guys, like Scott Pilgrim (Scott Pilgrim vs. the world) and Columbus (Zombieland) who are likable, intelligent and usually end up getting the girl. There's not really a female equivalent of that, so men know that they can be funny and charming and that's often enough, but girls know that if they're not also beautiful they're just not good enough. However, men have other problems which are just as damaging. There's an expectation that men will be tough and will not be emotional, with "man up" and "don't be a pussy" being among a couple of the many insults used to emasculate men for showing emotion. This deprives men from being able to open up about their emotions, and can even prevent some boys and men from seeking help for mental health problems. Speaking of which, there's a stereotype that only girls get eating disorders. While eating disorders are more common in girls, many boys also suffer, and are often overlooked due to the expectation that they couldn't have an eating disorder because they're a boy. So I do not want to overlook men's self-esteem, and I want to ensure that I address everyone, because self-esteem is important for everyone.
A problem with self-esteem in our society is that it tends to be linked to appearance. If a man doesn't look 'attractive', he better be very intelligent or very funny, and if a girl isn't attractive, she's just not as good as the 'pretty girls', no matter what she does. There have been some amazing campaigns to help tackle low-self esteem and body image problems. For example, Dove's capaign 'the evolution of a model' nicely demonstrates how many of the images we see of women are extensively photoshopped and do not even look like the models in the photo, let alone the average woman. This distorts the perception of what is attainable, and also of what is normal. When we are encouraged to strive for an unattainable ideal, we're obviously going to become dissapointed with ourselves. It's as though we've been given the goal of creating a perfect world, it just won't happen. Most people will not be able to look like models, most models don't look like models in real life. But everyone deserves to feel good about themselves, and everyone is beautiful is their own way. Instead of trying to strive for an unattainable goal, I think we should strive to broaden the goal. Beautiful should include people of all sizes, ages, races and gender identities. Who decided that being a size 6 was beautiful? Why can't a size 16 also be beautiful?
Above and beyond the idea of aesthetics, why don't be think about weight in terms of health? I mean, that's the only reason anyone should ever really need to change their weight. If you're having health problems due to being overweight, it's beneficial to lose weight. If you're having health problems from being underweight, you should put on weight. But if you're not having any problems, and you're within a healthy weight range, why should you have to worry about your weight? Isn't it odd that physical appearance is often put above health? Another thing which is odd is the perception of people as vein if they like the way that they look. For example, the lyrics "you don't know you're beautiful, and that's what makes you beautiful" (1D, ugh I know, you don't know you're beautiful) seem to represent the pervasive idea that it's 'cute' or 'desirable' for someone (especially a girl) to be insecure. It really shouldn't be. There's nothing bad about a person who is insecure, but insecurity shouldn't be encouraged, it sucks. Not liking yourself can take your attention away from school/work, it can make you not want to leave the house, it can make you feel very low and is just not fun. So, I'm askng people to please just try and accept that it's okay to like yourself, you should aim to love yourself.
Do I need treatment? What will happen if I get it?
It can be scary to admit that you need professional help for a mental health problem, and it can be difficult to decide whether or not you need help in the first place. For the most part, if you're thinking you might need help, you probably do. The biggest sign that you need help is if you have a psychological problem that is making everyday life difficult for you. For example, you might be struggling to complete work or go into school. You might be unable or unwilling to spend time with friends. If you're struggling with everyday tasks and your emotions/thoughts are having a significant negative impact on your life then you should seek professional help. I know it's scary, and sometimes its tricky to admit that you need help, but trust me when I say this, there is nothing to be embarrassed about and it is almost certainly the right choice. If you were suffering from a virus you'd go to the doctor, right? You should do the same thing when you have a mental health problem; the brain is an organ, it can get sick.
The NHS website has a lot of information on different mental health problems if you'd like to get an idea of what might be going on with the mental health of yourself or someone you're concerned about. I'll just give a little overview of the symptoms of a couple of common mental health problems.
Anxiety: anxiety is characterised by, well, anxiety. If you suffer from an anxiety disorder then you may feel on edge most of the time, find it difficult to relax, suffer from sleep disturbances (such as insomnia). You might have panic attacks, which are characterised by physical symptoms such as a racing heartbeat, shaking, sweating, headaches, feeling/being sick and having trouble breathing. Psychological symptoms of a panic attack include feeling like you're going to die. Anxiety can be generalised; where you basically feel on edge most of the time and can experience racing thoughts and feelings of anxiety for no obvious reason. It can also be more specific, such as social phobia; feeling anxious about social situations and finding it extremely distressing and difficult to be around people in certain situations. Anxiety can be treated, it is terrifying and can be debilitating at times, but (I reiterate) it can be treated. Common treatments include cognitive behavioural therapy (CBT) and medication. CBT involves challenging unhelpful thoughts around your anxiety. For example, you might be asked to conduct 'experiments' where you make a hypothesis about the worst thing that could happen in a particular situation, put yourself in the situation, and then (most of the time) see that the worst case scenario didn't happen. You may also be asked to come up with alternative thoughts and explanations for your anxiety. For example, if you're anxious because you think people will stare at you or judge you if you go out, you might come up with the alternative hypothesis that people will probably be more focused on themselves and what's happening in their own lives and most likely won't even notice you. Medications commonly prescriped for anxiety include antidepressants such as sertraline. These work by stopping the process of reuptake for the neurotransmitter serotonin, this basically means that more serotonin will be in your system. Since anxiety and depression are often co-morbid, treating depressive symptoms with antidepressants can be beneficial, these medications also often alleviate anxiety. Other medications for anxiety include benzodiazepines. These are sedatives/muscle relaxants which can often help with severe anxiety. You should discuss with your doctor whether or not you would like medication. There can be some unpleasant side-effects, such as headaches, sickness, and even (ironically) anxiety and suicidal thoughts (but these are very rare). Despite the side effects, most of these medications are very beneficial, especially when combined with CBT.
Depression: symptoms of depression include feelings of hopelessness and despair, guilt, sleep disturbances (insomnia or hypersomnia), loss of appetite or increased appetite and changes in weight, fatigue, psychomotor retardation (lack of movement and finding movement difficult), suicidal thoughts/plans of suicide, loss of pleasure and desires (you might stop enjoying things that you used to love, you might not feel any pleasure from food or sex), Dr. Robert Sapolsky has referred to it as "no longer being able to enjoy the sunrise" (his lecture on depression is very informative if you want to learn more https://www.youtube.com/watch?v=NOAgplgTxfc). You might also experience physical pain such as sickness and aching in your muscles. If you have mild depression, your doctor might recommend self-help, such as exercise and using self-help books and meditation. These methods can be useful for mild depression, but if you have moderate or severe depression you will need more help than this, and if your mild depression lasts more than a few weeks you will need further help. Further help can come in the form of CBT and medication. Common medications include flouxetine (prozac), zoloft, citalopram and sertraline. The most effective treatment for depression is a combination of CBT and medication. A word of warning, though, it might take you some time to find the right medication for you, so you should be patient and persevere. If you're experiencing suicidal thoughts and/or have plans of suicide then you should get immediate help. Go to A&E or call 999, someone will be there to help you. Sub-types of depression include psychotic depression, in which you will also experience psychotic symptoms such as delusions (unreasonable/untrue beliefs) and/or hallucinations (seeing things that aren't there). If you experience psychotic symptoms you will also probably be prescribed antipsychotic medication. Psychosis can be very, very scary, but it is treatable. Because people experiencing psychosis often do not realise their thoughts/experiences are not real, they might not seek help by themselves. If you think someone you know is suffering from psychotic symptoms you should persuade them to see their doctor as soon as possible, and if the symptoms are severe and/or they may be a danger to themselves or others then you should take them to the hospital.
Eating disorders: Types of eating disorders include anorexia, bulimia and binge-eating disorder. Each of these have one thing in common; disturbed patterns of eating and negative/overwhelming emotions surrounding food. You may experience changes in weight (extreme weight loss in anorexia, weight gain in binge-eating disorder). If you are having severe/persistent anxiety around eating you may be suffering from anorexia. If you intentionally starve yourself/restrict your calories, then you will need help. If you eat large amounts of food at once and feel out of control whilst eating then you may suffer from binge-eating disorder, you might also experience severe guilt/sadness after binging. If you follow binges with episodes of purging (compensatory behaviour such as vomiting, using laxetive medication and/or intense exercise) then you may be suffering from bulimia. Because eating disorders are very physically damaging, and have one of the highest mortality rates of any mental illness, it is important that you get help quickly if you have any signs of an eating disorder. The earlier you get help the more likely you are to recover. The treatment I got for my ED was CBT at the child and adolescent mental health service (CAMHS) and then hospitalization. It's scary to be hospitalized, but if your ED is severe and/or you are having physical problems because of it (such as low potassium, severely low weight, etc.) it might be necessary for you to be treated in hospital. The doctors are there to help you, even though you may feel like they are demons. If you have anorexia and are refusing to eat then you may be given a feeding tube. This will most likely be very distressing, but I promise you that doctors do not give people feeding tubes unless they have to. If you have very low potassium due to vomiting or starvation you may be given an IV drip, trust me, it will make you feel better. All of these physical interventions are only given when they are necessary. Even though it might feel like the doctors and nurses around you are being awful, and doing all of these things you don't want them to do, I promise they are trying to help you. If you have a danerously low BMI you will be required to gain weight. This might sound like a nightmare, but it is a necessary part of recovery. You won't be made to suddenly gain a bunch of weight; it will be gradual and controlled, and you should be fully supported during your entire recovery. When you are physically better psychological treatments such as CBT and medication are also much more effective.
I've talked about a few mental health problems people might be suffering from, if any of the descriptions fit you then you should get help. Your first port of call should be your GP, unless you are having a psychological crisis (such as suicidal thoughts), in which case you should go to the hospital. Your GP will be able to refer you to the appropriate services, who will then conduct an assesment of your psychological state and will discuss with you treatment options. It's scary to reach out, but I can promise you that mental health services are there to help you, and getting help is always the right thing. You deserve to feel well in body and mind.
It can be scary to admit that you need professional help for a mental health problem, and it can be difficult to decide whether or not you need help in the first place. For the most part, if you're thinking you might need help, you probably do. The biggest sign that you need help is if you have a psychological problem that is making everyday life difficult for you. For example, you might be struggling to complete work or go into school. You might be unable or unwilling to spend time with friends. If you're struggling with everyday tasks and your emotions/thoughts are having a significant negative impact on your life then you should seek professional help. I know it's scary, and sometimes its tricky to admit that you need help, but trust me when I say this, there is nothing to be embarrassed about and it is almost certainly the right choice. If you were suffering from a virus you'd go to the doctor, right? You should do the same thing when you have a mental health problem; the brain is an organ, it can get sick.
The NHS website has a lot of information on different mental health problems if you'd like to get an idea of what might be going on with the mental health of yourself or someone you're concerned about. I'll just give a little overview of the symptoms of a couple of common mental health problems.
Anxiety: anxiety is characterised by, well, anxiety. If you suffer from an anxiety disorder then you may feel on edge most of the time, find it difficult to relax, suffer from sleep disturbances (such as insomnia). You might have panic attacks, which are characterised by physical symptoms such as a racing heartbeat, shaking, sweating, headaches, feeling/being sick and having trouble breathing. Psychological symptoms of a panic attack include feeling like you're going to die. Anxiety can be generalised; where you basically feel on edge most of the time and can experience racing thoughts and feelings of anxiety for no obvious reason. It can also be more specific, such as social phobia; feeling anxious about social situations and finding it extremely distressing and difficult to be around people in certain situations. Anxiety can be treated, it is terrifying and can be debilitating at times, but (I reiterate) it can be treated. Common treatments include cognitive behavioural therapy (CBT) and medication. CBT involves challenging unhelpful thoughts around your anxiety. For example, you might be asked to conduct 'experiments' where you make a hypothesis about the worst thing that could happen in a particular situation, put yourself in the situation, and then (most of the time) see that the worst case scenario didn't happen. You may also be asked to come up with alternative thoughts and explanations for your anxiety. For example, if you're anxious because you think people will stare at you or judge you if you go out, you might come up with the alternative hypothesis that people will probably be more focused on themselves and what's happening in their own lives and most likely won't even notice you. Medications commonly prescriped for anxiety include antidepressants such as sertraline. These work by stopping the process of reuptake for the neurotransmitter serotonin, this basically means that more serotonin will be in your system. Since anxiety and depression are often co-morbid, treating depressive symptoms with antidepressants can be beneficial, these medications also often alleviate anxiety. Other medications for anxiety include benzodiazepines. These are sedatives/muscle relaxants which can often help with severe anxiety. You should discuss with your doctor whether or not you would like medication. There can be some unpleasant side-effects, such as headaches, sickness, and even (ironically) anxiety and suicidal thoughts (but these are very rare). Despite the side effects, most of these medications are very beneficial, especially when combined with CBT.
Depression: symptoms of depression include feelings of hopelessness and despair, guilt, sleep disturbances (insomnia or hypersomnia), loss of appetite or increased appetite and changes in weight, fatigue, psychomotor retardation (lack of movement and finding movement difficult), suicidal thoughts/plans of suicide, loss of pleasure and desires (you might stop enjoying things that you used to love, you might not feel any pleasure from food or sex), Dr. Robert Sapolsky has referred to it as "no longer being able to enjoy the sunrise" (his lecture on depression is very informative if you want to learn more https://www.youtube.com/watch?v=NOAgplgTxfc). You might also experience physical pain such as sickness and aching in your muscles. If you have mild depression, your doctor might recommend self-help, such as exercise and using self-help books and meditation. These methods can be useful for mild depression, but if you have moderate or severe depression you will need more help than this, and if your mild depression lasts more than a few weeks you will need further help. Further help can come in the form of CBT and medication. Common medications include flouxetine (prozac), zoloft, citalopram and sertraline. The most effective treatment for depression is a combination of CBT and medication. A word of warning, though, it might take you some time to find the right medication for you, so you should be patient and persevere. If you're experiencing suicidal thoughts and/or have plans of suicide then you should get immediate help. Go to A&E or call 999, someone will be there to help you. Sub-types of depression include psychotic depression, in which you will also experience psychotic symptoms such as delusions (unreasonable/untrue beliefs) and/or hallucinations (seeing things that aren't there). If you experience psychotic symptoms you will also probably be prescribed antipsychotic medication. Psychosis can be very, very scary, but it is treatable. Because people experiencing psychosis often do not realise their thoughts/experiences are not real, they might not seek help by themselves. If you think someone you know is suffering from psychotic symptoms you should persuade them to see their doctor as soon as possible, and if the symptoms are severe and/or they may be a danger to themselves or others then you should take them to the hospital.
Eating disorders: Types of eating disorders include anorexia, bulimia and binge-eating disorder. Each of these have one thing in common; disturbed patterns of eating and negative/overwhelming emotions surrounding food. You may experience changes in weight (extreme weight loss in anorexia, weight gain in binge-eating disorder). If you are having severe/persistent anxiety around eating you may be suffering from anorexia. If you intentionally starve yourself/restrict your calories, then you will need help. If you eat large amounts of food at once and feel out of control whilst eating then you may suffer from binge-eating disorder, you might also experience severe guilt/sadness after binging. If you follow binges with episodes of purging (compensatory behaviour such as vomiting, using laxetive medication and/or intense exercise) then you may be suffering from bulimia. Because eating disorders are very physically damaging, and have one of the highest mortality rates of any mental illness, it is important that you get help quickly if you have any signs of an eating disorder. The earlier you get help the more likely you are to recover. The treatment I got for my ED was CBT at the child and adolescent mental health service (CAMHS) and then hospitalization. It's scary to be hospitalized, but if your ED is severe and/or you are having physical problems because of it (such as low potassium, severely low weight, etc.) it might be necessary for you to be treated in hospital. The doctors are there to help you, even though you may feel like they are demons. If you have anorexia and are refusing to eat then you may be given a feeding tube. This will most likely be very distressing, but I promise you that doctors do not give people feeding tubes unless they have to. If you have very low potassium due to vomiting or starvation you may be given an IV drip, trust me, it will make you feel better. All of these physical interventions are only given when they are necessary. Even though it might feel like the doctors and nurses around you are being awful, and doing all of these things you don't want them to do, I promise they are trying to help you. If you have a danerously low BMI you will be required to gain weight. This might sound like a nightmare, but it is a necessary part of recovery. You won't be made to suddenly gain a bunch of weight; it will be gradual and controlled, and you should be fully supported during your entire recovery. When you are physically better psychological treatments such as CBT and medication are also much more effective.
I've talked about a few mental health problems people might be suffering from, if any of the descriptions fit you then you should get help. Your first port of call should be your GP, unless you are having a psychological crisis (such as suicidal thoughts), in which case you should go to the hospital. Your GP will be able to refer you to the appropriate services, who will then conduct an assesment of your psychological state and will discuss with you treatment options. It's scary to reach out, but I can promise you that mental health services are there to help you, and getting help is always the right thing. You deserve to feel well in body and mind.

Coping with binge/purge urges
It can be truly awful when you've got that nagging voice in your head telling you to do what you know you shouldn't. It's especially frustrating if you've been doing well, as it can feel like a set-back. Believe it or not, though, it is perfectly normal for someone with an ED like bulimia to get these urges, and it's not something to feel guilty about (that won't help anything). It's difficult to resist the urges when they're strong, but it is very possible. Here are some things that I've found useful in recovery which might be helpful to others...
1. Distraction: a lot of the time binge/purge urges go away with time, even when it feels like they're just too strong to ever go away. One of the best things you can do is take yourself out of that situation and distract yourself from the impulse to binge/purge. Try doing something active, such as going for a walk (but DO NOT use exercise as a purging method/coping strategy). Doing something creative can be very useful as it requires mental energy and attention, which means you won't be thinking about bingeing/purging as much. Make sure it's something you enjoy and something that requires effort/thinking, that way you'll be more distracted.
2. Talking: having a conversation with someone you love/trust about your feelings can be very useful. Being able to get out your frustrations and anxieties can be relieving, as can the realization that the people around you want to help and care about you. If you don't feel able to speak about your urges, just having a casual conversation with a friend can be helpful; it can boost your mood and also be part of a distraction. Oh, and make sure it's a funny friend, laughter helps.
3. Get it out: scream, punch a pillow, rant and rave. Get out your emotions in a non-harmful way. This can be relieving, and can help get rid of the anxieties/frustrations surrounding binge/purge urges. It's okay to admit to feeling a bit shit as long as you don't let it set you back in your recovery.
4. Figure out why: sometimes certain things can trigger binge/purge urges. Watching TV shows about dieting/weight, looking at magazines with pictures of unrealistic bodies, eating foods that you associate with bingeing, these can all be triggering. Once you know the reason for your feelings, it can be easier to deal with them, as you can understand where your feelings come from. If you know your triggers, you can also avoid them. A word of warning, however, avoiding 'fear foods' because they trigger bingeing/purging can be the right thing in the short term, but for long-term recovery it is necessary to challenge yourself and eat foods you find scary without bingeing/purging. Just do it when you're ready, and with the help of trusted others who can make sure you do it safely.
Hopefully some of these tips will prove useful and help others get through binge/purge urges. The most important thing to remember is that they do pass, as horrible as they can be, and each time you don't give in to them increases your chances of staying healthy.
It can be truly awful when you've got that nagging voice in your head telling you to do what you know you shouldn't. It's especially frustrating if you've been doing well, as it can feel like a set-back. Believe it or not, though, it is perfectly normal for someone with an ED like bulimia to get these urges, and it's not something to feel guilty about (that won't help anything). It's difficult to resist the urges when they're strong, but it is very possible. Here are some things that I've found useful in recovery which might be helpful to others...
1. Distraction: a lot of the time binge/purge urges go away with time, even when it feels like they're just too strong to ever go away. One of the best things you can do is take yourself out of that situation and distract yourself from the impulse to binge/purge. Try doing something active, such as going for a walk (but DO NOT use exercise as a purging method/coping strategy). Doing something creative can be very useful as it requires mental energy and attention, which means you won't be thinking about bingeing/purging as much. Make sure it's something you enjoy and something that requires effort/thinking, that way you'll be more distracted.
2. Talking: having a conversation with someone you love/trust about your feelings can be very useful. Being able to get out your frustrations and anxieties can be relieving, as can the realization that the people around you want to help and care about you. If you don't feel able to speak about your urges, just having a casual conversation with a friend can be helpful; it can boost your mood and also be part of a distraction. Oh, and make sure it's a funny friend, laughter helps.
3. Get it out: scream, punch a pillow, rant and rave. Get out your emotions in a non-harmful way. This can be relieving, and can help get rid of the anxieties/frustrations surrounding binge/purge urges. It's okay to admit to feeling a bit shit as long as you don't let it set you back in your recovery.
4. Figure out why: sometimes certain things can trigger binge/purge urges. Watching TV shows about dieting/weight, looking at magazines with pictures of unrealistic bodies, eating foods that you associate with bingeing, these can all be triggering. Once you know the reason for your feelings, it can be easier to deal with them, as you can understand where your feelings come from. If you know your triggers, you can also avoid them. A word of warning, however, avoiding 'fear foods' because they trigger bingeing/purging can be the right thing in the short term, but for long-term recovery it is necessary to challenge yourself and eat foods you find scary without bingeing/purging. Just do it when you're ready, and with the help of trusted others who can make sure you do it safely.
Hopefully some of these tips will prove useful and help others get through binge/purge urges. The most important thing to remember is that they do pass, as horrible as they can be, and each time you don't give in to them increases your chances of staying healthy.

What not to say to someone with an eating disorder (and some things you should say)
Sometimes it’s tricky to approach the subject of mental health with the people around you, especially if you’re worried about theirs. Here’s a run down of things you probably shouldn’t say if you want to help someone with an eating disorder:
1. (This one refers to Anorexia) “Just eat”- not helpful. Not at all. This will probably just make the person upset and/or withdraw from you. Having an eating disorder is not a choice, and people cannot just ‘snap out’ of them and get better instantaneously. If they could ‘just eat’ they would. A similar one referring to Bulimia and Binge-Eating Disorder is “Just don’t think about food/don’t binge”. I want to slow clap and become annoyingly sarcastic when people say things like that. This idea has not eluded the person with an eating disorder (ED). They won’t suddenly think “Oh, right, I shouldn’t do that”. They know. A better thing to say might be “Please try and wait before you binge” or “If you still want to binge in an hour, ok, but for now sit with me/distract yourself”. This can be extremely helpful, as often a binge craving can subside with time. Having the support and encouragement to try and let it pass can give someone the strength to start getting better. Fair warning, though, when people are deep in an ED they may not be responsive and may become angry when you try to change their behaviours. I know from experience that sometimes you’re just not ready to get better. In these cases, professional help and time may be needed before the above statement can become helpful.
2. “You’re bringing everyone down/you’re worrying me”- it’s tempting, I know. If you’re a close friend or relative of someone with an ED this can be terrifying. It’s awful to see someone you care about harming themselves like that. However, the likelihood is that the person you’re concerned about knows you’re worried and feels incredibly guilty about that. The thing is, they will almost definitely be using their ED to cope with negative feelings, including guilt. This will become a vicious cycle. The thing to remember is that us folks with ED’s don’t want to worry anyone around us, most of the time we’ll try to hide it. We don’t mean to hurt you, and the reminder that we are will probably just fuel our negative self-esteem. A better way to approach this might be to say something like: “I’m concerned about you; can you talk about it?”. This way, you’re expressing your concern without pushing blame on the person and giving them the option to speak about it.
3. “You’re so difficult”- this is one of the worst. The thing is, being particular about food is very, very different from having and ED. Even when we’re in recovery there may be certain foods we won’t feel comfortable eating, or certain situations we won’t be able to participate in. I, for example, still need to count calories and find it very, very difficult (basically impossible) to eat at a restaurant unless they have nutritional information. So, even though I’m doing a lot, lot better and am basically recovered, there’s still things I just can’t do. Now, for people still in the midst of an ED, it’s even harder. They’re not being ‘difficult’ or ‘picky’, they are having extreme anxiety around food which can be paralysing. Also, for those with Bulimia or Anorexia-binge-purge-subtype, pushing someone to eat something they are not comfortable with might be a trigger for a binge/purge. This is, obviously, not good. Sometimes, in order to stay healthy, it is important for a person with/recovering from an ED to know their limits and only push themselves when they feel ready. It would be much better to simply ask the person with an ED what would make it easier for them. If they need calorie information and you can provide it, that’s a problem easily solved. If they’re just too overwhelmed to deal with the situation, let them know they don’t have to do anything they don’t want to do. Trust me, we appreciate that.
The most important thing to remember is that if you’re trying you’re best to be supportive, and you’re listening to the person you’re concerned about, then you’re doing good. It can be difficult to know how to help someone with a mental health issue, especially when it’s as physically damaging as an ED, but at the end of the day, a little support and understanding goes a long way.
Sometimes it’s tricky to approach the subject of mental health with the people around you, especially if you’re worried about theirs. Here’s a run down of things you probably shouldn’t say if you want to help someone with an eating disorder:
1. (This one refers to Anorexia) “Just eat”- not helpful. Not at all. This will probably just make the person upset and/or withdraw from you. Having an eating disorder is not a choice, and people cannot just ‘snap out’ of them and get better instantaneously. If they could ‘just eat’ they would. A similar one referring to Bulimia and Binge-Eating Disorder is “Just don’t think about food/don’t binge”. I want to slow clap and become annoyingly sarcastic when people say things like that. This idea has not eluded the person with an eating disorder (ED). They won’t suddenly think “Oh, right, I shouldn’t do that”. They know. A better thing to say might be “Please try and wait before you binge” or “If you still want to binge in an hour, ok, but for now sit with me/distract yourself”. This can be extremely helpful, as often a binge craving can subside with time. Having the support and encouragement to try and let it pass can give someone the strength to start getting better. Fair warning, though, when people are deep in an ED they may not be responsive and may become angry when you try to change their behaviours. I know from experience that sometimes you’re just not ready to get better. In these cases, professional help and time may be needed before the above statement can become helpful.
2. “You’re bringing everyone down/you’re worrying me”- it’s tempting, I know. If you’re a close friend or relative of someone with an ED this can be terrifying. It’s awful to see someone you care about harming themselves like that. However, the likelihood is that the person you’re concerned about knows you’re worried and feels incredibly guilty about that. The thing is, they will almost definitely be using their ED to cope with negative feelings, including guilt. This will become a vicious cycle. The thing to remember is that us folks with ED’s don’t want to worry anyone around us, most of the time we’ll try to hide it. We don’t mean to hurt you, and the reminder that we are will probably just fuel our negative self-esteem. A better way to approach this might be to say something like: “I’m concerned about you; can you talk about it?”. This way, you’re expressing your concern without pushing blame on the person and giving them the option to speak about it.
3. “You’re so difficult”- this is one of the worst. The thing is, being particular about food is very, very different from having and ED. Even when we’re in recovery there may be certain foods we won’t feel comfortable eating, or certain situations we won’t be able to participate in. I, for example, still need to count calories and find it very, very difficult (basically impossible) to eat at a restaurant unless they have nutritional information. So, even though I’m doing a lot, lot better and am basically recovered, there’s still things I just can’t do. Now, for people still in the midst of an ED, it’s even harder. They’re not being ‘difficult’ or ‘picky’, they are having extreme anxiety around food which can be paralysing. Also, for those with Bulimia or Anorexia-binge-purge-subtype, pushing someone to eat something they are not comfortable with might be a trigger for a binge/purge. This is, obviously, not good. Sometimes, in order to stay healthy, it is important for a person with/recovering from an ED to know their limits and only push themselves when they feel ready. It would be much better to simply ask the person with an ED what would make it easier for them. If they need calorie information and you can provide it, that’s a problem easily solved. If they’re just too overwhelmed to deal with the situation, let them know they don’t have to do anything they don’t want to do. Trust me, we appreciate that.
The most important thing to remember is that if you’re trying you’re best to be supportive, and you’re listening to the person you’re concerned about, then you’re doing good. It can be difficult to know how to help someone with a mental health issue, especially when it’s as physically damaging as an ED, but at the end of the day, a little support and understanding goes a long way.
Recovery Guilt
Ok, so I’m not sure how many other people experience this, but I occasionally get a weird, sinking feeling of guilt when I realise how well I’m doing. I’m well into recovery now, and probably wouldn’t be recognised by my old counsellors, and this sometimes makes me feel a bit…bad. It doesn’t logically make sense, of course, but I feel as though I am faking my mental illness. When I find myself able to eat something which once would have terrified me, like, god forbid, chocolate, I feel as though perhaps I’ve made a big fuss of nothing. When I find myself able to do things which would once have panicked me, like talk to a shop keeper, I think that perhaps I was never really anxious, and I feel guilty because I wonder if I’ve concocted a big mess in my head over nothing.
I’m not sure how common this feeling is, but I have a theory. I think our society has a bit of a binary view of mental health; you’re ill or you’re not. But the problem is, many people are in the middle, and recovery is a process of travelling through the spectrum from mentally ill to healthy. So, when we start to get better, perhaps we see ourselves as no longer mentally ill. Now, we know that’s not possible; you don’t just go from mentally ill to healthy like that, so we get cognitive dissonance, and convince ourselves that we were lying.
I think getting better is weird; you change a lot about yourself and sometimes have to live in a very different way. It’s hard, and on top of that there’s a lot of inherent conflict in recovering; there’s usually a part of you that doesn’t want to. Here we move on to my second theory; brains can be bitches. I think that sometimes when we have a mental illness it can become like a comfort blanket, and we don’t want to let it go. If we want to be anthropomorphic we could also say that mental illnesses don’t want us to get better from them (it can feel that way at times). For that reason, our brain may create a feeling of guilt in order to encourage us to continue with destructive behaviours to ‘prove’ to ourselves that we are actually ill. Dick-ish, right? Well, that’s the subconscious for you.
So, maybe it’s because society tells us we’re either ill or we’re not, and so if we’re able to do good sometimes we must be faking it. Or maybe it’s because a part of us doesn’t want to let our mental illness go. Either way, guilt about recovery is obviously not good. It can put some real obstacles in the way of getting better. It’s hard enough to try and overcome the compulsions, feelings and thoughts that come with mental illness, let alone worrying that you’ve been exaggerating when things get better. The fact of the matter is, just because you can cope better now doesn’t mean you don’t still have problems to face. It’s like if you’ve broken a leg; it’ll get better as it heals, but it’ll take time, and once it’s healed that doesn’t take away from the fact that it was broken. Or maybe, more accurately, it’s like if you have a chronic illness; you might need to take medication to keep it under control. Just because the medication is working doesn’t mean you lied to the doctor when you described your symptoms.
Ok, so I’m not sure how many other people experience this, but I occasionally get a weird, sinking feeling of guilt when I realise how well I’m doing. I’m well into recovery now, and probably wouldn’t be recognised by my old counsellors, and this sometimes makes me feel a bit…bad. It doesn’t logically make sense, of course, but I feel as though I am faking my mental illness. When I find myself able to eat something which once would have terrified me, like, god forbid, chocolate, I feel as though perhaps I’ve made a big fuss of nothing. When I find myself able to do things which would once have panicked me, like talk to a shop keeper, I think that perhaps I was never really anxious, and I feel guilty because I wonder if I’ve concocted a big mess in my head over nothing.
I’m not sure how common this feeling is, but I have a theory. I think our society has a bit of a binary view of mental health; you’re ill or you’re not. But the problem is, many people are in the middle, and recovery is a process of travelling through the spectrum from mentally ill to healthy. So, when we start to get better, perhaps we see ourselves as no longer mentally ill. Now, we know that’s not possible; you don’t just go from mentally ill to healthy like that, so we get cognitive dissonance, and convince ourselves that we were lying.
I think getting better is weird; you change a lot about yourself and sometimes have to live in a very different way. It’s hard, and on top of that there’s a lot of inherent conflict in recovering; there’s usually a part of you that doesn’t want to. Here we move on to my second theory; brains can be bitches. I think that sometimes when we have a mental illness it can become like a comfort blanket, and we don’t want to let it go. If we want to be anthropomorphic we could also say that mental illnesses don’t want us to get better from them (it can feel that way at times). For that reason, our brain may create a feeling of guilt in order to encourage us to continue with destructive behaviours to ‘prove’ to ourselves that we are actually ill. Dick-ish, right? Well, that’s the subconscious for you.
So, maybe it’s because society tells us we’re either ill or we’re not, and so if we’re able to do good sometimes we must be faking it. Or maybe it’s because a part of us doesn’t want to let our mental illness go. Either way, guilt about recovery is obviously not good. It can put some real obstacles in the way of getting better. It’s hard enough to try and overcome the compulsions, feelings and thoughts that come with mental illness, let alone worrying that you’ve been exaggerating when things get better. The fact of the matter is, just because you can cope better now doesn’t mean you don’t still have problems to face. It’s like if you’ve broken a leg; it’ll get better as it heals, but it’ll take time, and once it’s healed that doesn’t take away from the fact that it was broken. Or maybe, more accurately, it’s like if you have a chronic illness; you might need to take medication to keep it under control. Just because the medication is working doesn’t mean you lied to the doctor when you described your symptoms.

Overthinking: how to cope
So, it's two in the morning and you're living up to the Twenty One Pilots lyrics from Ride "I been thinking too much". Well, I'll help you. Overthinking is a common trap to fall into, even for people without mental health issues, and for those with problems such as anxiety, it is very common. Symptoms include running over the same thoughts in your mind multiple times, going over old conversations, and even events from years in the past. It can lead to anxiety penetrating your body, making you feel on edge and uncomfortable. It tends to make sleep very difficult. If this is something that you deal with, then you've probably tried many things to stop the pattern of thinking too much; lavender, sleeping pills, counting sheep, telling yourself to stop (the least useful of all of these). If none of these have helped, then I have some tips for you which may help alleviate some of your struggle.
Tip 1: Have a shower or bath before bed. This can help relax your muscles and get your body ready for rest. Having candles and music can also help to put your mind at ease and distract you from unwanted thoughts. Making this part of a bedtime routine can also help separate the day from the night, classically conditioning you to associate baths/showers with being ready for bed.
Tip 2: Write down your concerns and thoughts in the morning and before bed. This can help you to express your thoughts and get out any worries, meaning that you may be less inclined to turn over distressing thoughts in your head while you are trying to sleep. This can also be useful for your mental health in general, as being able to express your emotions in a controlled and healthy way can mean you are less likely to have pent up emotions and anxieties.
Tip 3: Have noise in the background. If you are having trouble sleeping at night because of unwanted thoughts, then having music or television on in the background can be very helpful. It means that your thoughts have less of your attention, and gives you something else to focus on. It can also be comforting, especially if you are listening to something that reminds you of good times or that makes you happy.
Tip 4: Distract yourself. If you are finding yourself overthinking during the day, distracting yourself by doing something you enjoy or removing yourself from the situation can be very useful. Even a change of scenery by going for a walk can be very useful. Having fresh air and the sunlight on your face can sometimes be enough to take away harsh thoughts and calm you down. Having a hobby, such as drawing or writing, or even watching films, can be a great way to distract yourself when you are overthinking. So don yourself in a blanket and get that popcorn, being a couch potato is sometimes all you need. But if you're more of a gym bunny, there's good news, exercise releases endorphin's and can work as an antidepressant, so it can be a very useful way to distract yourself from worries and put yourself in a good mood.
Tip 5: Figure out why you're overthinking. Write down all of the thoughts you have when you think too much, and the worries that consume you. You may find a pattern which could lead you to the route of your overthinking. Sometimes just knowing what's causing something can make it easier to cope with.
One of the most important things to do is talk to someone; having a friend or family member you can confide in can take some of the burden off your own shoulders and make it easier to cope when your brain wants to make you think about everything that could go wrong. If your overthinking is intruding on your life and making it difficult for you to cope with everyday things then it may be necessary to see a professional. This can be scary, but counselors have heard it all, and they're only there to help.
So, it's two in the morning and you're living up to the Twenty One Pilots lyrics from Ride "I been thinking too much". Well, I'll help you. Overthinking is a common trap to fall into, even for people without mental health issues, and for those with problems such as anxiety, it is very common. Symptoms include running over the same thoughts in your mind multiple times, going over old conversations, and even events from years in the past. It can lead to anxiety penetrating your body, making you feel on edge and uncomfortable. It tends to make sleep very difficult. If this is something that you deal with, then you've probably tried many things to stop the pattern of thinking too much; lavender, sleeping pills, counting sheep, telling yourself to stop (the least useful of all of these). If none of these have helped, then I have some tips for you which may help alleviate some of your struggle.
Tip 1: Have a shower or bath before bed. This can help relax your muscles and get your body ready for rest. Having candles and music can also help to put your mind at ease and distract you from unwanted thoughts. Making this part of a bedtime routine can also help separate the day from the night, classically conditioning you to associate baths/showers with being ready for bed.
Tip 2: Write down your concerns and thoughts in the morning and before bed. This can help you to express your thoughts and get out any worries, meaning that you may be less inclined to turn over distressing thoughts in your head while you are trying to sleep. This can also be useful for your mental health in general, as being able to express your emotions in a controlled and healthy way can mean you are less likely to have pent up emotions and anxieties.
Tip 3: Have noise in the background. If you are having trouble sleeping at night because of unwanted thoughts, then having music or television on in the background can be very helpful. It means that your thoughts have less of your attention, and gives you something else to focus on. It can also be comforting, especially if you are listening to something that reminds you of good times or that makes you happy.
Tip 4: Distract yourself. If you are finding yourself overthinking during the day, distracting yourself by doing something you enjoy or removing yourself from the situation can be very useful. Even a change of scenery by going for a walk can be very useful. Having fresh air and the sunlight on your face can sometimes be enough to take away harsh thoughts and calm you down. Having a hobby, such as drawing or writing, or even watching films, can be a great way to distract yourself when you are overthinking. So don yourself in a blanket and get that popcorn, being a couch potato is sometimes all you need. But if you're more of a gym bunny, there's good news, exercise releases endorphin's and can work as an antidepressant, so it can be a very useful way to distract yourself from worries and put yourself in a good mood.
Tip 5: Figure out why you're overthinking. Write down all of the thoughts you have when you think too much, and the worries that consume you. You may find a pattern which could lead you to the route of your overthinking. Sometimes just knowing what's causing something can make it easier to cope with.
One of the most important things to do is talk to someone; having a friend or family member you can confide in can take some of the burden off your own shoulders and make it easier to cope when your brain wants to make you think about everything that could go wrong. If your overthinking is intruding on your life and making it difficult for you to cope with everyday things then it may be necessary to see a professional. This can be scary, but counselors have heard it all, and they're only there to help.
Depression
Do you marvel at the beauty of a sunrise? Or the intricate details of your new lace dress or fancy suit?
Do you feel your heart racing when you think of your crush?
Do you get that warm feeling of satisfaction when you complete a goal?
Do you get excited and motivated by your goals, and your future, because when I'm depressed I don't.
And that's what I miss the most.
Depression isn't just sadness, sometimes it's nothing.
It can be like waiting for a train that never comes, or waiting to receive a gift that doesn't even exist.
It can be like being static, stuck, just going though the motions.
It's knowing you should be worried about your grades or your job, but not feeling anything.
It's getting something you always wanted, and finding that you can't even smile.
It's not sadness, but the absence of happiness and pleasure, that I think is the worst part.
But I'm lucky, I do get moment's of reprieve and clarity, and I have people around me, and I do have hope and an ability to understand my issues.
I want to spare a thought for those who have it so much worse, and have no help, and I want to ask them not to give up.
Do you marvel at the beauty of a sunrise? Or the intricate details of your new lace dress or fancy suit?
Do you feel your heart racing when you think of your crush?
Do you get that warm feeling of satisfaction when you complete a goal?
Do you get excited and motivated by your goals, and your future, because when I'm depressed I don't.
And that's what I miss the most.
Depression isn't just sadness, sometimes it's nothing.
It can be like waiting for a train that never comes, or waiting to receive a gift that doesn't even exist.
It can be like being static, stuck, just going though the motions.
It's knowing you should be worried about your grades or your job, but not feeling anything.
It's getting something you always wanted, and finding that you can't even smile.
It's not sadness, but the absence of happiness and pleasure, that I think is the worst part.
But I'm lucky, I do get moment's of reprieve and clarity, and I have people around me, and I do have hope and an ability to understand my issues.
I want to spare a thought for those who have it so much worse, and have no help, and I want to ask them not to give up.

Anxiety Coping Techniques
Anxiety can come in different forms, and anxiety is not always a sign of a disorder. For example, it would be perfectly rational to be anxious when faced with a murderous lunatic welding an axe. However, where Anxiety Disorders, such as Generalized Anxiety Disorder and Social Anxiety, differ from simple stress or everyday anxiety, is the fact that they often involve the person suffering becoming irrationally anxious.
They will find themselves experiencing the instinctive fight or flight response that is synonymous with fear when in a situation that does not present any real danger, but is perceived by the sufferers brain as dangerous.
The fight or flight response is one of humanities evolutionally tools, and is is wonderfully useful for our bodies, as it allows our adrenaline to begin pumping around our system so that we can run from threats.
However, in our modern world where predators are no longer lurking around every corner and we have little need for this response, anxiety can become somewhat of a problem.
What you are experiencing during a panic attack is the result of the adrenaline which courses through your body during the fight or flight response, having nowhere to go. Your elevated heartbeat and heavy breathing is due to the fact that the extra energy and adrenaline your body now has is not actually needed. This can leave you breathing heavily, feeling dizzy and shaky, as well as feeling weak.
This experience can be very scary, and in itself a panic attack can induce further anxiety because it can, as in my case, cause what is often referred to as dissociation or de-realization. This is where you can feel as though you are not real, or even that you are dreaming, and you may find yourself losing touch with reality.
Symptoms of Anxiety Disorders that can be noticed by outsiders include isolation, as some of those suffering from Anxiety may find themselves scared of going outside, and in extreme cases may develop Agoraphobia. Other symptoms include heavy breathing, elevated heart rate, sweaty palms, and light headedness. ufferers are at a higher risk of developing other mental health problems such as OCD, depression and Self-Injury. This is because most mental health problems can come in the form of overlaps of different conditions. For example, it would be perfectly understandable for someone with psychosis to then become paranoid or to develop anxiety, due to the fact that they seeing images that others claim not too, and having auditory hallucinations that are understandably unsettling.
Anxiety disorders are often very difficult to overcome, as the horrific feeling of dread that comes with these conditions can be overwhelming, however, there are things that can be done to overcome and manage these feelings. One of the most helpful things when faced with a diagnosis of anxiety, is to identify the causes and triggers of your anxious feelings. This not only allows you to understand that what you are feeling is in fact anxiety, a treatable and common condition that many people deal with, but also allows you to avoid triggering situations or understand the reasons why you feel anxious in order to overcome this.
Many common triggers include social situations, where it is common to worry that people are speaking about you or laughing at you. Whilst this can be distressing, and at the time that these feelings are occurring it can be difficult to rationalize with yourself, there are strategies that can be used to overcome this. For example, a strategy that has greatly helped me is self-talk, I must simply remind myself of the lives of the strangers around me, and of how tiny a part I have in their lives.
This allows me to remember that it would be strange of them to pay enough attention to me to laugh at me or talk about me behind my back, as they surely have more to do in their lives than this, and if they do not, then that is none of my concern.
It should be remembered that often when we feel anxious we are in no real danger.
It can be useful to take a moment to simply focus on your breathing, on the small usually discarded sounds around you, and remember that you are ok, and the feelings of anxiety will eventually pass.
Another strategy that can be very useful is called grounding. This involves taking a moment to focus on your surroundings and your senses. If you are outside it may be a good idea to focus on the cold air around you, or the warm summer breeze. If you are listening to music or the television you may want to focus on how the sound waves feel when they go past your ears, or focus on the background sounds that compliment the music or the voices from your television.
Search around you, and try to spot everything in your surroundings. You may wish to try and see how many objects of a certain color you have, or count the number of books you own. One of the most helpful grounding techniques I have found is using things such as scented candles and bath bombs to surround myself in a comforting cocoon of sweet smells.
Whatever your preference, this technique is especially good for those whose anxiety gives them feelings of disassociation, and makes it seem as though they are not real. It is also an especially good technique for avoiding self-injury as it allows you to stimulate your dopamine receptors as well as distract yourself from how you feel without having to panic or harm yourself.
It is important for anxiety sufferers to have support, if you have not spoken about your feelings to your loved ones, or you feel that you have no-one in your life that you trust enough to speak to about these things, it can be very difficult to find help. However, there are many things that you can do to find support.
CAMHS is a mental health service for adolescents that can help, you may wish to call them on 01273 718680. If you do not like the idea of speaking to professionals, then you may wish to go on YouTube, where many self-help youtuber’s have made helpful videos, such as Laura Lejeune and Melissa Seawater, as well as other channels.
You can always go to Horsesmouth.co.uk, an online mentoring network, where I also mentor as XxRiaxX and will always be willing to talk. There are a lot of helpful people who all have their own experiences and will not judge you, as it is likely that if you are talking to a mentor on the website, they have probably experienced similar things.
There are many websites like this online where people will talk to you and help you if you need it. If you are feeling desperate then calling someone like Child line or the Samaritans may help, as someone can talk you down and give you some time to get your feelings out.
The best thing to do, if possible, is to talk to someone in your life that you trust and that can help you, this will mean you can get support and you wont be holding your feelings in anymore. I am aware that it can be really scary, because there is always the worry of being judged or thought of as silly, but those who love you are likely to have noticed that something is wrong, as people close to those with anxiety often notice that they are unhappy but do not know why or what to do.
They may be relieved when you speak to them, and happy that you felt you could tell them, as well as happy that there is a reason for your behavior or visible anxiety.
The main thing to remember is that having anxiety is not your fault, nor is it something that you should or can control. It is something that can be managed, a medical condition much like diabetes or asthma that you should never be ashamed of and should aim to manage, not ‘cure’.
Those with anxiety, depression or any mental illness have the ability to live a happy and successful life with the right support, and that is the most important thing to remember. Things can be horrible one moment, and can seem hopeless, but life changes, times goes on, and things will get better.
Anxiety can come in different forms, and anxiety is not always a sign of a disorder. For example, it would be perfectly rational to be anxious when faced with a murderous lunatic welding an axe. However, where Anxiety Disorders, such as Generalized Anxiety Disorder and Social Anxiety, differ from simple stress or everyday anxiety, is the fact that they often involve the person suffering becoming irrationally anxious.
They will find themselves experiencing the instinctive fight or flight response that is synonymous with fear when in a situation that does not present any real danger, but is perceived by the sufferers brain as dangerous.
The fight or flight response is one of humanities evolutionally tools, and is is wonderfully useful for our bodies, as it allows our adrenaline to begin pumping around our system so that we can run from threats.
However, in our modern world where predators are no longer lurking around every corner and we have little need for this response, anxiety can become somewhat of a problem.
What you are experiencing during a panic attack is the result of the adrenaline which courses through your body during the fight or flight response, having nowhere to go. Your elevated heartbeat and heavy breathing is due to the fact that the extra energy and adrenaline your body now has is not actually needed. This can leave you breathing heavily, feeling dizzy and shaky, as well as feeling weak.
This experience can be very scary, and in itself a panic attack can induce further anxiety because it can, as in my case, cause what is often referred to as dissociation or de-realization. This is where you can feel as though you are not real, or even that you are dreaming, and you may find yourself losing touch with reality.
Symptoms of Anxiety Disorders that can be noticed by outsiders include isolation, as some of those suffering from Anxiety may find themselves scared of going outside, and in extreme cases may develop Agoraphobia. Other symptoms include heavy breathing, elevated heart rate, sweaty palms, and light headedness. ufferers are at a higher risk of developing other mental health problems such as OCD, depression and Self-Injury. This is because most mental health problems can come in the form of overlaps of different conditions. For example, it would be perfectly understandable for someone with psychosis to then become paranoid or to develop anxiety, due to the fact that they seeing images that others claim not too, and having auditory hallucinations that are understandably unsettling.
Anxiety disorders are often very difficult to overcome, as the horrific feeling of dread that comes with these conditions can be overwhelming, however, there are things that can be done to overcome and manage these feelings. One of the most helpful things when faced with a diagnosis of anxiety, is to identify the causes and triggers of your anxious feelings. This not only allows you to understand that what you are feeling is in fact anxiety, a treatable and common condition that many people deal with, but also allows you to avoid triggering situations or understand the reasons why you feel anxious in order to overcome this.
Many common triggers include social situations, where it is common to worry that people are speaking about you or laughing at you. Whilst this can be distressing, and at the time that these feelings are occurring it can be difficult to rationalize with yourself, there are strategies that can be used to overcome this. For example, a strategy that has greatly helped me is self-talk, I must simply remind myself of the lives of the strangers around me, and of how tiny a part I have in their lives.
This allows me to remember that it would be strange of them to pay enough attention to me to laugh at me or talk about me behind my back, as they surely have more to do in their lives than this, and if they do not, then that is none of my concern.
It should be remembered that often when we feel anxious we are in no real danger.
It can be useful to take a moment to simply focus on your breathing, on the small usually discarded sounds around you, and remember that you are ok, and the feelings of anxiety will eventually pass.
Another strategy that can be very useful is called grounding. This involves taking a moment to focus on your surroundings and your senses. If you are outside it may be a good idea to focus on the cold air around you, or the warm summer breeze. If you are listening to music or the television you may want to focus on how the sound waves feel when they go past your ears, or focus on the background sounds that compliment the music or the voices from your television.
Search around you, and try to spot everything in your surroundings. You may wish to try and see how many objects of a certain color you have, or count the number of books you own. One of the most helpful grounding techniques I have found is using things such as scented candles and bath bombs to surround myself in a comforting cocoon of sweet smells.
Whatever your preference, this technique is especially good for those whose anxiety gives them feelings of disassociation, and makes it seem as though they are not real. It is also an especially good technique for avoiding self-injury as it allows you to stimulate your dopamine receptors as well as distract yourself from how you feel without having to panic or harm yourself.
It is important for anxiety sufferers to have support, if you have not spoken about your feelings to your loved ones, or you feel that you have no-one in your life that you trust enough to speak to about these things, it can be very difficult to find help. However, there are many things that you can do to find support.
CAMHS is a mental health service for adolescents that can help, you may wish to call them on 01273 718680. If you do not like the idea of speaking to professionals, then you may wish to go on YouTube, where many self-help youtuber’s have made helpful videos, such as Laura Lejeune and Melissa Seawater, as well as other channels.
You can always go to Horsesmouth.co.uk, an online mentoring network, where I also mentor as XxRiaxX and will always be willing to talk. There are a lot of helpful people who all have their own experiences and will not judge you, as it is likely that if you are talking to a mentor on the website, they have probably experienced similar things.
There are many websites like this online where people will talk to you and help you if you need it. If you are feeling desperate then calling someone like Child line or the Samaritans may help, as someone can talk you down and give you some time to get your feelings out.
The best thing to do, if possible, is to talk to someone in your life that you trust and that can help you, this will mean you can get support and you wont be holding your feelings in anymore. I am aware that it can be really scary, because there is always the worry of being judged or thought of as silly, but those who love you are likely to have noticed that something is wrong, as people close to those with anxiety often notice that they are unhappy but do not know why or what to do.
They may be relieved when you speak to them, and happy that you felt you could tell them, as well as happy that there is a reason for your behavior or visible anxiety.
The main thing to remember is that having anxiety is not your fault, nor is it something that you should or can control. It is something that can be managed, a medical condition much like diabetes or asthma that you should never be ashamed of and should aim to manage, not ‘cure’.
Those with anxiety, depression or any mental illness have the ability to live a happy and successful life with the right support, and that is the most important thing to remember. Things can be horrible one moment, and can seem hopeless, but life changes, times goes on, and things will get better.
My Response To People Who Say "You're Too Fat To Have An Eating Disorder."
You're too fat to have an eating disorder. Too fat. Too fat. I'll just let that sink in for a moment before I explode with laughter and anger at the same time.
Ok, first of all, are you saying that binge eating disorder isn't an eating disorder? Because I'm pretty sure that if you binge you're not going to be sk
inny. Second of all, are you saying that anorexia is the only eating disorder that exists?
No, no, just no. People with anorexia usually lose weight and become drastically underweight, yes, but anorexia isn't the only eating disorder that exists. People with bulimia tend to maintain a healthy weight, or may even be a little overweight. People with binge eating disorder are generally overweight.
Eating disorders are categorized by an unhealthy relationship with food, allowing food to rule your life and not being able to maintain a healthy diet, not just by the weight a person is. Also, if someone has just developed the symptoms of anorexia they may appear to be a normal weight, but this doesn't mean that they don't have a problem.
It is a horribly unhelpful thing for people to say to those with eating disorders, because it causes self-consciousness and guilt about your own weight, and makes the person feel that the voices in their mind, if it is anorexia or bulimia, are right when they say that they are fat. Saying someone is too fat to have an eating disorder is ridiculous, that's like saying blonde people can't get depressed, it makes no sense.
To those who have been confronted with people like this I say, don't listen to them, it is you and your recovery that is most important, not what others say or think. Whatever weight you are is nothing to be ashamed of, people have different bodies, it's just the way it is, just focus on being healthy.
One last thing, when people say that 'real men like meat not bones' I understand that they are trying to encourage girls to be comfortable in their own skin, and I respect that, however, some girls are naturally skinny, and should not be made to feel bad about that. Also, even if a girl is skinny, even if she's not naturally skinny, its just as bad to criticise her for her weight than to criticise someone for being overweight or just above normal; its still judging on appearances, and causing potential emotional distress for others.
Some people don't look ill when they are, but you know what? Get over it. Some people look different, who cares? Some people have problems to deal with, that's their business, not yours to criticize. No-one has the right to say whether or not someone is going through a disorder when they know nothing about their situation.
Ok, first of all, are you saying that binge eating disorder isn't an eating disorder? Because I'm pretty sure that if you binge you're not going to be sk
inny. Second of all, are you saying that anorexia is the only eating disorder that exists?
No, no, just no. People with anorexia usually lose weight and become drastically underweight, yes, but anorexia isn't the only eating disorder that exists. People with bulimia tend to maintain a healthy weight, or may even be a little overweight. People with binge eating disorder are generally overweight.
Eating disorders are categorized by an unhealthy relationship with food, allowing food to rule your life and not being able to maintain a healthy diet, not just by the weight a person is. Also, if someone has just developed the symptoms of anorexia they may appear to be a normal weight, but this doesn't mean that they don't have a problem.
It is a horribly unhelpful thing for people to say to those with eating disorders, because it causes self-consciousness and guilt about your own weight, and makes the person feel that the voices in their mind, if it is anorexia or bulimia, are right when they say that they are fat. Saying someone is too fat to have an eating disorder is ridiculous, that's like saying blonde people can't get depressed, it makes no sense.
To those who have been confronted with people like this I say, don't listen to them, it is you and your recovery that is most important, not what others say or think. Whatever weight you are is nothing to be ashamed of, people have different bodies, it's just the way it is, just focus on being healthy.
One last thing, when people say that 'real men like meat not bones' I understand that they are trying to encourage girls to be comfortable in their own skin, and I respect that, however, some girls are naturally skinny, and should not be made to feel bad about that. Also, even if a girl is skinny, even if she's not naturally skinny, its just as bad to criticise her for her weight than to criticise someone for being overweight or just above normal; its still judging on appearances, and causing potential emotional distress for others.
Some people don't look ill when they are, but you know what? Get over it. Some people look different, who cares? Some people have problems to deal with, that's their business, not yours to criticize. No-one has the right to say whether or not someone is going through a disorder when they know nothing about their situation.
Eating Disorder Recovery Rules
These are a few things that I have found are extremely helpful in dealing with an eating disorder, I am writing it in order to advise anyone going through a mental health issue such as Anorexia, Bulimia or Binge Eating Disorder.
Now that’s out of the way, here’s my first rule, do things that make you happy. This is not only fun and an excuse to slack off, but also a scientifically valid method of dealing with any mental health problem. It is simple, when you do something that makes you happy, endorphins such as serotonin are released in the brain, and you end up smiling, or at least feeling better. It is particularly helpful in recovery because being happier means your coping mechanism is less necessary.
The second rule is that relapses are going to happen. If you have an eating disorder you have a chronic illness, like diabetes, you can’t just shrug it of, it will not work, but that is no reason to give up. If you relapse think to yourself that it is fine, you will do better tomorrow, and you will have just increased your chances of recovery.
The third rule is that food and/or weight loss will not ever bring you happiness in an eating disorder. It’s not like you're becoming healthier, or even more confident when you lose weight in an eating disorder. In fact, with anorexia especially; weight loss tends to coincide with increased depression, caused by the hormonal imbalances and lethargy that comes with not giving your body the nutrition it needs.
There are so many things that will bring you happiness in this life, and none of them involves being thinner, I can guarantee that. Also you need to remember that eating food for comfort will give you more issues to deal with, it is a quick solution that doesn't last nearly long enough to be worth it.
The fourth rule is to find the things that trigger you. This could be something as simple as a song that makes you sad, or a particular activity that puts you in a bad mood or makes you feel bad about yourself. Identifying things that trigger you to want to starve, binge, purge, or all three, is the first step towards avoiding them, and embracing recovery.
The fifth rule is to avoid triggering content. This can include food channels for anyone with Binge Eating Disorder or Bulimia. Thinspirations and fashion magazines are pretty much a bad thing for everyone, except the people who get paid for making them, so try to avoid them as much as possible; they will not make you feel better. If the things that trigger you are particular foods, and in Bulimia and Binge Eating Disorder this tends to be sugar filled sweets and fatty meals, then swapping them for something healthier may help you to gain control over your eating tendencies.
I understand that with eating disorders it is so tempting to immerse yourself in your illness. It seems easier, and I’ll admit that at first it might be, but in the long run you’ll just end up dead or tied to a hospital bed with a drip, so be brave and avoid the triggers as best you can, I pinky promise you won't regret it.
The sixth rule is to smash, or in less extreme cases simply get rid of, any scales you have been using. Scales are nothing but lying bastards that will not tell you anything about yourself. They can’t compliment you on your personality, or tell you how beautiful your eyes are; they can only present you with depressing numbers that will make you feel worthless. I know it can be addictive using scales, so if you find yourself squirming at the thought of completely getting rid of your scales, then you may want to consider using them less, and eventually you may feel ready to stop using them altogether.
The seventh rule is to celebrate any success. It can be as silly as being able to buy clothes without caring about the size, or as big as eating and keeping down a healthy meal, or avoiding a binge. All success is valid, and a good step towards feeling better. That’s what recovery is about, feeling better, feeling free, and feeling happy and strong, anyone who has been through a eating disorder and got through to the other side will tell you how much better life is after recovery.
The last rule is that if you have a therapist, listen to them, unless they're actually a terrible therapist, then get a new one. If you do not have any form of counseling, whilst it may seem frightening to reach out, it will be worth it if you can find someone helpful to talk to. I'm telling the truth, please believe me. The voice in your mind telling you that your fat, or giving you urges to binge, the voice driving you insane, is nothing but a liar. It will be difficult to shut it up, I’m not going to lie, it may be a daily struggle to ignore unhelpful thoughts, but if you can do it, then it will, and forgive me for sounding cliché, be the start of the rest of your life.
There are approximately seven billion people on this earth, it is inevitable that one of them thinks you're awesome, so listen to them and not the voices in your head.
Here are some helpful resources and youtuber’s:
http://www.youtube.com/user/idranktheseawater
http://www.youtube.com/user/Downtownpatrol
http://www.b-eat.co.uk
Now that’s out of the way, here’s my first rule, do things that make you happy. This is not only fun and an excuse to slack off, but also a scientifically valid method of dealing with any mental health problem. It is simple, when you do something that makes you happy, endorphins such as serotonin are released in the brain, and you end up smiling, or at least feeling better. It is particularly helpful in recovery because being happier means your coping mechanism is less necessary.
The second rule is that relapses are going to happen. If you have an eating disorder you have a chronic illness, like diabetes, you can’t just shrug it of, it will not work, but that is no reason to give up. If you relapse think to yourself that it is fine, you will do better tomorrow, and you will have just increased your chances of recovery.
The third rule is that food and/or weight loss will not ever bring you happiness in an eating disorder. It’s not like you're becoming healthier, or even more confident when you lose weight in an eating disorder. In fact, with anorexia especially; weight loss tends to coincide with increased depression, caused by the hormonal imbalances and lethargy that comes with not giving your body the nutrition it needs.
There are so many things that will bring you happiness in this life, and none of them involves being thinner, I can guarantee that. Also you need to remember that eating food for comfort will give you more issues to deal with, it is a quick solution that doesn't last nearly long enough to be worth it.
The fourth rule is to find the things that trigger you. This could be something as simple as a song that makes you sad, or a particular activity that puts you in a bad mood or makes you feel bad about yourself. Identifying things that trigger you to want to starve, binge, purge, or all three, is the first step towards avoiding them, and embracing recovery.
The fifth rule is to avoid triggering content. This can include food channels for anyone with Binge Eating Disorder or Bulimia. Thinspirations and fashion magazines are pretty much a bad thing for everyone, except the people who get paid for making them, so try to avoid them as much as possible; they will not make you feel better. If the things that trigger you are particular foods, and in Bulimia and Binge Eating Disorder this tends to be sugar filled sweets and fatty meals, then swapping them for something healthier may help you to gain control over your eating tendencies.
I understand that with eating disorders it is so tempting to immerse yourself in your illness. It seems easier, and I’ll admit that at first it might be, but in the long run you’ll just end up dead or tied to a hospital bed with a drip, so be brave and avoid the triggers as best you can, I pinky promise you won't regret it.
The sixth rule is to smash, or in less extreme cases simply get rid of, any scales you have been using. Scales are nothing but lying bastards that will not tell you anything about yourself. They can’t compliment you on your personality, or tell you how beautiful your eyes are; they can only present you with depressing numbers that will make you feel worthless. I know it can be addictive using scales, so if you find yourself squirming at the thought of completely getting rid of your scales, then you may want to consider using them less, and eventually you may feel ready to stop using them altogether.
The seventh rule is to celebrate any success. It can be as silly as being able to buy clothes without caring about the size, or as big as eating and keeping down a healthy meal, or avoiding a binge. All success is valid, and a good step towards feeling better. That’s what recovery is about, feeling better, feeling free, and feeling happy and strong, anyone who has been through a eating disorder and got through to the other side will tell you how much better life is after recovery.
The last rule is that if you have a therapist, listen to them, unless they're actually a terrible therapist, then get a new one. If you do not have any form of counseling, whilst it may seem frightening to reach out, it will be worth it if you can find someone helpful to talk to. I'm telling the truth, please believe me. The voice in your mind telling you that your fat, or giving you urges to binge, the voice driving you insane, is nothing but a liar. It will be difficult to shut it up, I’m not going to lie, it may be a daily struggle to ignore unhelpful thoughts, but if you can do it, then it will, and forgive me for sounding cliché, be the start of the rest of your life.
There are approximately seven billion people on this earth, it is inevitable that one of them thinks you're awesome, so listen to them and not the voices in your head.
Here are some helpful resources and youtuber’s:
http://www.youtube.com/user/idranktheseawater
http://www.youtube.com/user/Downtownpatrol
http://www.b-eat.co.uk
Suicidal Ideations And Self-Injury Recovery/Safety Rules
The first set of rules concern self-injury. The first one is a simple one, but something that is easy to overlook in a manic state. Take care of your wounds; this will reduce the risk of infection, and will help avoid a traumatic and embarrassing hospital visit, which if you do self-injure, you will probably appreciate.
The second self-injury rule is that you should attempt distraction. This is a technique which you have probably been told about so many times that the mere mention of it makes you wish to punch me in the face, but unfortunately I am not within your vicinity to be harmed, and the point is valid. If your self-injury is a coping technique, which it statistically is, then you can conclude that the emotions or events you are experiencing will pass with time, and so distracting yourself whilst you are going through this can be a brilliant help in avoiding the blade, fist or lighter.
The third self-injury rule is to have a support system. It is a terrifying and horrid thing to do, I understand, but telling someone you can rely on, if you know such a person, can greatly relieve your bottled up emotions, and be a step towards recovery. If you wish to get better, then a support system is most likely a necessity, as even if you genuinely want to stop, doing it by yourself is unfortunately almost impossible, as there will always be a part of you fighting for the addiction.
The fourth self-injury rule is that you must remember that habitual self-injury is an addiction, and should be treated as such. This is more for relatives and friends than anyone, if you treat someone you love who self-injures as though they are simply being irrational or stupid, you will do nothing but exacerbate the situation, and make them more isolated.
The fifth self-injury rule is to avoid veins as best you can. Going too deep can be a death sentence, or can leave you passed out on the bathroom floor, and that is not a situation anyone wants to be in. being safe is vital if you self-injure, it can be the difference between eventual recovery and permanent physical and mental damage. Bad experiences in self-injury can in fact make the habit worse, as they add more things to cope with in your mind, and so avoiding them, and attempting to create some warmer memories can be a great help.
The last self-injury rule is to not be ashamed of your scars, if you are still creating new ones, or if you manage to recover. Having faded scars is not something to be embarrassed about, it proves that you were strong enough to kick self-injury’s ass. Having new scars is also nothing to be ashamed of, it is nothing to be proud of, but it is what it is, don’t let it pull you deeper into the addiction, and definitely do not let it isolate you from the world, that won’t do any good. You have not done anything wrong, you have simply attempted to cope with a situation that got to much for you, and that makes you nothing but human.
The second set of rules concern suicidal ideations. The first suicidal ideation rule is to keep it that way. What I mean by this is that even if you are having suicidal thoughts, you do not need to become actively suicidal. If you have not yet made plans, that is a great sign, keep it that way, I beg you.
The second suicidal ideation rule is that if you do ever cross over to being actively suicidal, and make plans, then as hard as it may be, resist carrying them out, or tell someone about it so that you can get the appropriate help. If you ignore this, or simply cannot bring yourself to speak out, and believe me that is understandable, then I am afraid your future will have been lost, and believe me you have one. Statistics will tell you that things cannot stay negative forever, if they have been getting worse recently, or have hit rock bottom, then soon they will be on their way back up, and you must try to remain brave until then.
The third suicidal ideation rule is to write down all of the things that give you happiness in life, no matter how small they are. This can be big things like your family and friends, or small things like your favorite foods and drinks, your favorite movie or music, or just the sound of rain hitting your window. Hopefully when you can realize that there are so many good things in life, even if they are small, you will be able to put the bad things into perspective.
Above all, please don't give up.
The second self-injury rule is that you should attempt distraction. This is a technique which you have probably been told about so many times that the mere mention of it makes you wish to punch me in the face, but unfortunately I am not within your vicinity to be harmed, and the point is valid. If your self-injury is a coping technique, which it statistically is, then you can conclude that the emotions or events you are experiencing will pass with time, and so distracting yourself whilst you are going through this can be a brilliant help in avoiding the blade, fist or lighter.
The third self-injury rule is to have a support system. It is a terrifying and horrid thing to do, I understand, but telling someone you can rely on, if you know such a person, can greatly relieve your bottled up emotions, and be a step towards recovery. If you wish to get better, then a support system is most likely a necessity, as even if you genuinely want to stop, doing it by yourself is unfortunately almost impossible, as there will always be a part of you fighting for the addiction.
The fourth self-injury rule is that you must remember that habitual self-injury is an addiction, and should be treated as such. This is more for relatives and friends than anyone, if you treat someone you love who self-injures as though they are simply being irrational or stupid, you will do nothing but exacerbate the situation, and make them more isolated.
The fifth self-injury rule is to avoid veins as best you can. Going too deep can be a death sentence, or can leave you passed out on the bathroom floor, and that is not a situation anyone wants to be in. being safe is vital if you self-injure, it can be the difference between eventual recovery and permanent physical and mental damage. Bad experiences in self-injury can in fact make the habit worse, as they add more things to cope with in your mind, and so avoiding them, and attempting to create some warmer memories can be a great help.
The last self-injury rule is to not be ashamed of your scars, if you are still creating new ones, or if you manage to recover. Having faded scars is not something to be embarrassed about, it proves that you were strong enough to kick self-injury’s ass. Having new scars is also nothing to be ashamed of, it is nothing to be proud of, but it is what it is, don’t let it pull you deeper into the addiction, and definitely do not let it isolate you from the world, that won’t do any good. You have not done anything wrong, you have simply attempted to cope with a situation that got to much for you, and that makes you nothing but human.
The second set of rules concern suicidal ideations. The first suicidal ideation rule is to keep it that way. What I mean by this is that even if you are having suicidal thoughts, you do not need to become actively suicidal. If you have not yet made plans, that is a great sign, keep it that way, I beg you.
The second suicidal ideation rule is that if you do ever cross over to being actively suicidal, and make plans, then as hard as it may be, resist carrying them out, or tell someone about it so that you can get the appropriate help. If you ignore this, or simply cannot bring yourself to speak out, and believe me that is understandable, then I am afraid your future will have been lost, and believe me you have one. Statistics will tell you that things cannot stay negative forever, if they have been getting worse recently, or have hit rock bottom, then soon they will be on their way back up, and you must try to remain brave until then.
The third suicidal ideation rule is to write down all of the things that give you happiness in life, no matter how small they are. This can be big things like your family and friends, or small things like your favorite foods and drinks, your favorite movie or music, or just the sound of rain hitting your window. Hopefully when you can realize that there are so many good things in life, even if they are small, you will be able to put the bad things into perspective.
Above all, please don't give up.
